Hi, welcome to the site. Good question. We “sort” of know it - but I believe it likely varies by cell type and by person. We know from the scientific literature that rapamycin binds very specifically to mTORC1, and indirectly to mTORC2:
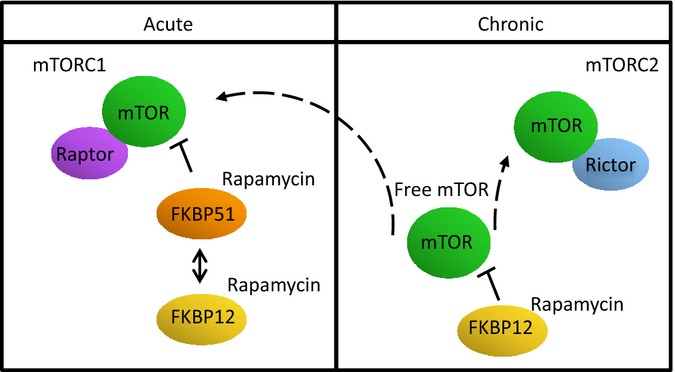
It is well established that rapamycin directly inhibits mTORC1 through a noncompetitive mechanism by establishing a three-way interaction with mTOR and FKBP12 (Liang et al ., 1999). While rapamycin binds mTORC1 directly, it does not bind the mTORC2 complex. Instead, it is proposed that rapamycin inhibits the assembly of the mTORC2 complex in a manner requiring FKBP12.
The general operating model that the researchers are using is that mTORC1 inhibition drives the benefits that we see (anti-aging) but the mTORC2 inhibition drives the negative side effects. This is not proven completely - but its the general model that the researchers say they are working on.
We also know that to get the immune system modulation (which for us would be a negative side effect, but is their goal) that the organ transplant patients get when they take high dosages of rapamycin can require much higher dosages, for longer periods of time.
Anecdotally at a personal level we see most people taking and you can see the benefits they are suggesting at these levels, and the side effects (which all seem pretty benign):
But what we don’t know is how the doses impact (or will impact) any given individual - both from a blood level response, and a side effect (or benefits in detail) perspective.
The research is still early in anti-aging, and very little has been done on rapamycin in generally healthy individuals (as opposed to really sick people - cancer… organ transplantation, etc. and who are typically taking many different medications in addition to rapamycin.
although this paper didn’t seem to quantify the degree of inhibition of MTORC2, the photo figures showed a strong response. It does seem wise to take some time off of R to let any inhibited metabolism return to normal for a while.
Agreed… its probably wise to take periodic “vacations” from rapamycin to pause any possible mTORC2 inhibition. Of course - the big issue is when and for how long?
I wonder if there are any potential leading indicators that your mTORC2 is getting too inhibited? I also wonder if it matters (in humans) where (in what organs and tissues) and when the mTORC2 inhibition is taking place? And if that might be revealed in any way short of tissue biopsies.
From that same paper first referenced above:
" As expected, inhibition of the phosphorylation of the mTORC1 substrate, S6 (S240/244), was seen in every tissue tested, but mTORC2 inhibition, measured by the phosphorylation of Akt (S473), was only seen to differing degrees in a subset of tissues including heart, soleus muscle, gastrocnemius muscle, pancreas, liver, lung, visceral fat, and spleen (Figs(Figs6A6A,,BB,,CC and S3)"
Obviously, much more research needs to be done on the mTORC2 inhibition issue, and how pulse dosing may or may not inhibit mTORC2 over weeks, months and years. All the literature talks about the need for “chronic” and typically “high” dosing of rapamycin to inhibit mTORC2 - but the exact definitions of “chronic” seems to lack experimental evidence in healthy humans especially related to periodic schedules.
In some tissues/diseases, such as cancer, it will likely be beneficial to inhibit both mTORC1 and mTORC2 where others, such as the aging process in general, might benefit from mTORC1-selective inhibition to avoid the negative metabolic side effects associated with prolonged treatment of the drug (Stallone et al ., 2009; Houde et al ., 2010). Current literature supports that the inhibition of mTORC1 contributes to the longevity effects of rapamycin and the inhibition of mTORC2, specifically in the liver, causes the negative effects of rapamycin on glucose homeostasis. However, more experiments are required to understand how the inhibition of these 2 complexes on a tissue-by-tissue basis affects the longevity of the organism as a whole.
I’m just reviewing more on the whole issue of mTORC2 inhibition as its an important area I’m still learning about. Here are some notes from a podcast with one of the Novartis authors of the 2014 Mannick paper:
Peter Attia asked Lloyd Klickstein:
How much exposure to rapamycin before you start to see this dual-prong of inhibition of TORC1 and TORC2?
His response was:
In humans, after a week to a month, you can start to see consequences of TORC2 inhibition with a rapalog alone and it’s reflected in hyperglycemia and hypertriglyceridemia. This happens in “normal” people as well—i.e., non-diabetic, non-immunocompromised
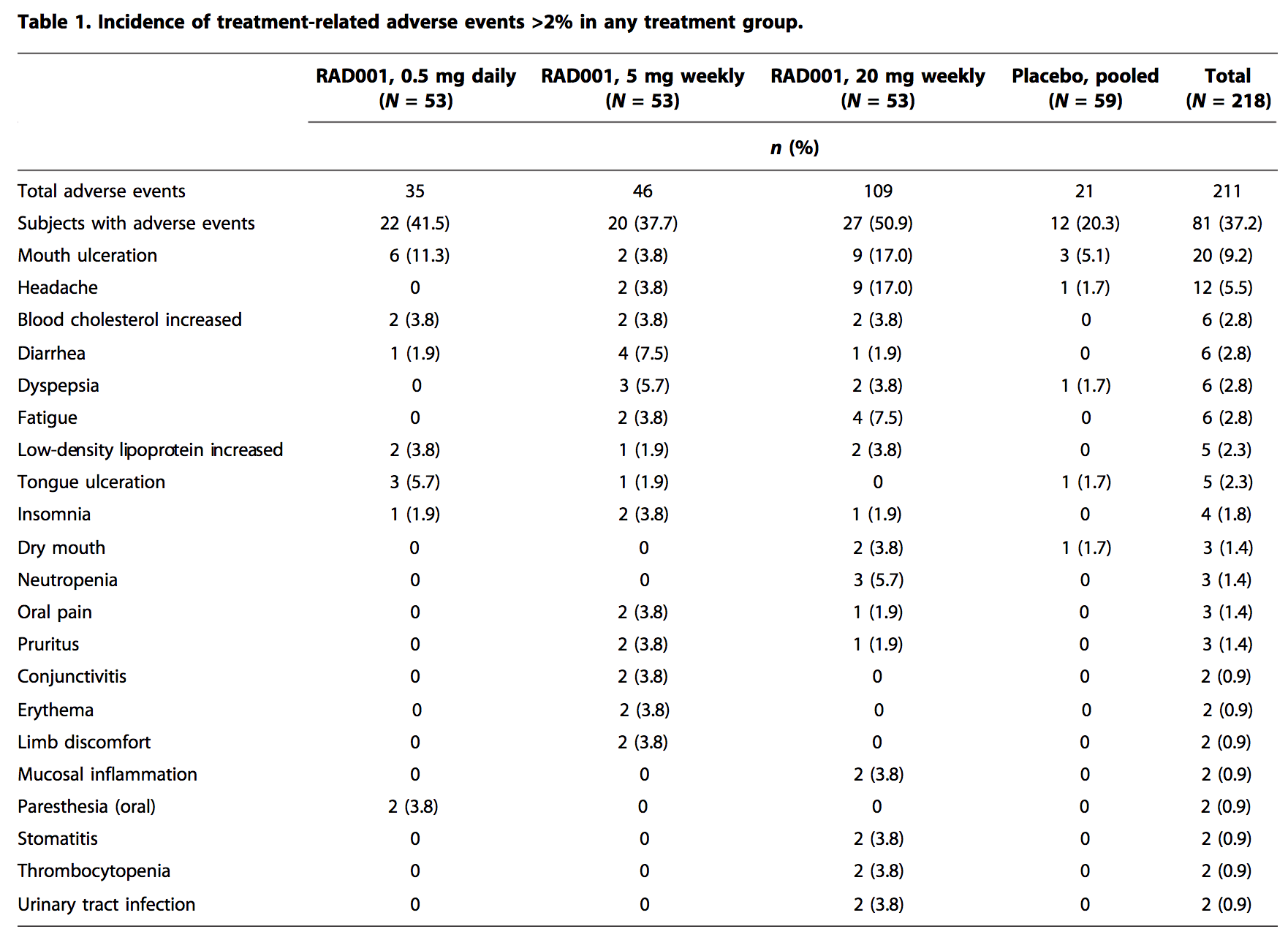
In one experiment. Patients with polycystic kidney disease that were otherwise healthy, took the rapalog (RAD001) and a substantial fraction saw these biochemical changes in their blood
The dose was 5 to 10 mg a day (equivalent to 2-8 mg of rapamycin)
BUT… not everyone has these effects and that it unclear why that’s the case
Again - in this example the doses are very high - 5mg to 10mg PER DAY - for weeks or month+.
Additionally - there is significant controversy over the interpretation of the “hyperglycemia and hypertriglyceridemia” mentioned above. Many researchers - Matt Kaeberlein and Mikhail Blaggosklony, included - who believe that these are benign effects that are part of the lifespan extension effect.
Green mentions 2 weeks to allow rapa 62 hr half life to decrease blood level then re-dose.
Green mentioned on top of the desire to suppress mtor, he used the words: benefit of rapa is also due to a differential between blood level now vs post dose. I add the words; spiking, pulsing. VS continuously keep mtor supressed. Just attempting to bring Dr Green comments here. Best to all.
Wondering if there is any research or anecdotal information about rapamycin and resistance exercise. It seems pretty clear that while rapamycin supplementation reduces muscle wasting (sarcopenia) in aging mice, it also blocks protein synthesis. Since I do both cardio and resistance training, I wonder if one should schedule resistance training at 1. the end of the week after taking sirolimus or 2. during the washout vacation period? See
Interesting question regarding the differentiated issue of cardio and resistance training. I also do both - biking for an hour 3 or 4 times a week, and strength training 2 or 3 times a week for 45 minutes or so. I don’t change my schedule based on my rapamycin intake - but I do expect different results.
From what I’ve read, in the first few days after rapamycin intake you likely have much higher mTOR inhibition - so muscle growth after workout will likely be minimized. But - I think it was discussed by Peter Attia and Matt Kaeberlein in their recent podcast, or perhaps another one - generally the theory is just keep exercising on your regular schedule, and you’ll get some benefit. When mTOR is highly inhibited your workout will help to maintain your muscle and help prevent muscle wasting (due to lack of mTOR) - and then when the mTOR inhibition has receded - i.e. later in the week, you’ll get more gains.
On the broader issue of strength training / muscle building and rapamycin use - did you see this previous conversation?
I initially worried about rapamycin inhibiting muscle growth. However, something I read recently (frustrated that I didn’t record source) said that taking rapamycin periodically will enhance muscle growth because the periods of autophagy will enable the anabolic phase to work better.
thank you. after doing research and thinking about rapamycin for 2 years, i just took my first dose this morning. i went straight to 5mg of rapamune, figuring that this is probably the minimum effective dose, and can go to 6mg next week. i have done 3 day fasts several times, so i figured that i have some experience with inhibiting mtor the natural way. other then a small headache the first hour (very likely a placebo type of effect), i feel totally normal. i also put on a glucose monitor for the next two weeks to see if anything changes from my norm.
I just checked my ketones, as rapa seems to be somewhat of a fasting memetic, and is supposed to increase utilization of fatty acids. i was at 0.7mmol which is fairly low and may just be a result of not really eating much carbs today. (on a 3 day fast, i can hit on day 3 4-6mmol)
Oh wow, I jsut had some carbs (not a lot), about 11 hours after taking 5mg, and my glucose response was MUCH higher (around 40 points higher then where it should be after what I ate) the normal. Based on this I will be extra careful with carbs when at peak dosage, and maybe add back metformin or take acarbose when eating a carby meal.
I would highly recommend that people take a look at their post prandial glucose levels after dosing rapa
As a Type 1 diabetic, I keep a close eye on my blood glucose, and I have noticed no discernible effect of rapa. In fact, my blood glucose may be slightly lower during the first couple of days after dosing rapa.
i am not diabetic, but i find that its lower when on rapa if not eating carbs or at night its much flatter then normal. but when eating carbs, the response it more extreme, but comes down quickly.
i would assume that its similar to in a fasted state. when fasting and there are fatty acids at the muscles, they dont take up glucose as well (the glute 4 transporter get inhibited from intaking glucose into the muscle). the most likely reason is to preserve the glucose for the brain.