I’ve got a long research deep dive, but don’t know how to post it. I’m a new member with restrictions.
I’d maybe start a new thread. I will join because I’ve an interest in senolytics.
I have bumped up your status, please try to post it.
This is a paper on the impact of retatrutide on kidney function : The Effect of Retatrutide on Kidney Parameters in Participants With Type 2 Diabetes Mellitus and/or Obesity - PMC
This is based on phase 2 clinical data. Here’s how this aligns with the strategies mentioned by the paper above (summary courtesy of AI) :
1. Mitigation of “Inflammaging” and Oxidative Stress
The first paper identifies chronic systemic inflammation and oxidative stress as primary drivers of kidney dysfunction. The retatrutide study demonstrates that this triple agonist significantly reduces Urine Albumin-to-Creatinine Ratio (UACR)—a key marker of kidney damage—by up to 43% in patients with type 2 diabetes and 26% in those with obesity.
- Mechanism: While the primary effect is metabolic (weight loss and glucose control), the paper notes that GLP-1 and glucagon receptor agonism may exert direct anti-inflammatory and anti-oxidative effects on renal cells, potentially slowing the inflammatory cascades that lead to senescence.
2. Targeting Mitochondrial Health and Metabolism
The first paper highlights mitochondrial dysfunction as a “pillar” of aging. Retatrutide’s unique inclusion of glucagon receptor agonism specifically targets metabolic efficiency.
- Energy Balance: By stimulating glucagon receptors, retatrutide may increase energy expenditure and fatty acid oxidation. This helps resolve “lipotoxicity” (the accumulation of toxic fats in the kidney), which the first paper identifies as a trigger for cellular stress and the Senescence-Associated Secretory Phenotype (SASP).
3. Preserving Renal Function
The review paper focuses on the kidney as a model for aging, emphasizing the need for therapies that preserve the Estimated Glomerular Filtration Rate (eGFR).
- Renoprotection: The retatrutide study found that eGFR remained stable or showed slight, clinically insignificant increases over 36–48 weeks. This suggests a “renoprotective” profile that could prevent the accelerated decline typical of immunosenescence and chronic kidney disease.
4. Systemic Risk Reduction
The inflammaging paper argues for multimodal therapies that address multiple age-related diseases simultaneously.
- Multimodal Impact: Retatrutide fits this “multimodal” requirement by simultaneously addressing obesity, glycemic control, and blood pressure. By improving these systemic factors, it reduces the overall “metabolic friction” that accelerates cellular aging and systemic inflammation across multiple organ systems, not just the kidney.
Why were these EGFR increases considered “clinically insignificant”?
The paper provides several reasons why these small increases in eGFR are viewed positively or neutrally rather than as a sign of kidney stress:
- Stability of Cystatin C: When the researchers used Cystatin C (an alternative biomarker for kidney function that is less affected by muscle mass than creatinine), the eGFR values were even more stable. This suggests that some of the “increase” seen in creatinine-based eGFR might be related to the significant weight loss (and potential change in muscle mass) rather than a change in the kidney’s filtering units.
- Lack of Hyperfiltration: Pathological hyperfiltration (which can damage the kidney over time) is usually much more pronounced. The modest 3–4 ml/min increase is consistent with what has been observed in other GLP-1 receptor agonist trials, which have historically shown long-term kidney protection.
- Correlation with UACR Improvement: Because these small eGFR increases occurred alongside significant decreases in albuminuria (UACR)—up to 43%—the researchers interpreted the overall effect as “renoprotective” (kidney-protecting) rather than harmful.
3 Likes
I don’t understand this, it’s highly selective and has no effect on cells that are not in a state of senescence. The DRI aspect of this peptide matters.
I think having a high level of senescent cells is scary, compared to reducing them and the SASP they secrete.
Off the top of my head, keep in mind a couple facts,
- you cannot eliminate all senescent cells
- senolytics do not stop new senescent cells from being produced
- Senescent cells are continually created on demand
- the immune system is the primary way senescent cells are naturally “managed”
- senescent cells are harder to clear as we age, due to aging immune system’
- there are many senescent cell types, each with common and unique properties
- Each senescent cell type as a SASP fingerprint
- SASP has over 500 cytokines, chemokines, etc, depending on the senescent cell type
- 4 secretions have been identified as having a recruiting function, making nearby cells become senescent, even when they are healthy cells
- senescent cells count eventually goes exponential as we age
- in damaged vertebral discs, biopsies and autopsies “old people” have shown that as much as 60% of the cells are useless senescent cells
Senescent cells have an effect on 8 of the 12 Hallmarks of Aging. The next closest one is Mitochondrial disfunction with an effect on 7 of the Hallmarks.
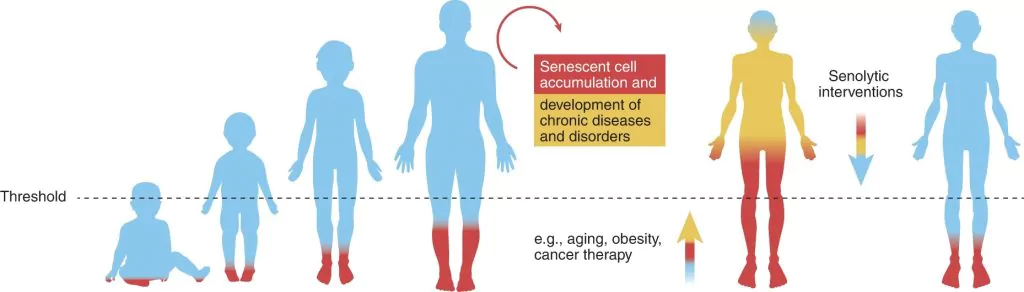
Reducing senescent cells to a “healthy level”, the Threshold of Senescence, is proposed as one of the better way to increase Health Span.
I have no interest in the “life span” debates. I’m only interested in being healthy until I die.
2 Likes
Amen, brother.
1 Like
A chronic, sterile (non-bacterial) inflammation that increases with age. It is predicted by markers like IL-6 , TNF-α , and CRP .
I wonder when I see these associations, does is follow that low hsCRP implies low kidney inflammation?
The issue is that in the research the past few years they’ve discovered that there is a lot of variation in the types of senescent cells, in different organs, etc. So you can’t have a generic “senolytic”… there will be many, and this is where the companies are moving. See this presentation: Highlights from the 2023 Longevity Summit - #4 by RapAdmin
1 Like
I just started a new tread in the forum dedicated to a FOXO4-DRI discussion. I posted my research summary deep dive into FOXO4-DRI. It is obviously a fascinating idea and the mouse study was really attention grabbing.
But there a bunch of ways senescent (and senescent appearing) cell apoptosis can kill you. Mostly we do not know much. As much of the biology as I understand is in the note I posed in the new thread.
Let’s continue any discussion there. I’d love to be just a little less convinced the unknown risks do not justify the unknown benefits.
1 Like
Since I use nearly 50 mg for 2 people in one cycle that source would cost $1,875.00
This is not new and has been mentioned at least as far back as 2015.
With over 240 cell types, of which over 200 can become senescent it was known then that there were at least 2 pathways SNC’s used to remain immortal by defeating the immune system and the apoptotic system to remain immortal.
I don’t believe that regular methods used by most people to increase autophagy/apoptosis have much effect on SNC’s. The science of senescence doesn’t support that.
Neutralizing the “immortality” enabling function(s) appears to be the most common way of clearing SNC’s
When I first became interested in zombie cells, in 2018, this was already known and the D+Q protocol studies indicated this combo acts against the p16^INK4a^/Rb‑positive senescent cells
FOX04-DRI activates the p53/BCL‑2/Caspase‑3 apoptotic pathway
I used my version of the D+Q protocol for 6 years, 4 cycles per year.
Now I’m adding the FOX04-DRI protocol twice a year to address the other types of senescent cells.
Do or do not, there is no try ![]()
So I do.
Also there is this
Many senescent cell types co‑express p53 activity and p16^INK4a^/Rb markers and simultaneously require both the p53‑mediated apoptotic priming and BCL‑2‑mediated survival signals to resist death. Consequently, a single senescent cell—e.g., a senescent fibroblast or endothelial cell in skin or vasculature—can be susceptible to both FOXO4‑DRI (via p53 re‑activation) and D+Q (via BCL‑2 inhibition) .
Because the two senolytics peak in apoptotic activity at slightly different times (FOXO4‑DRI ~48‑72 h, D+Q ~24‑48 h) , a staggered schedule (e.g., FOXO4‑DRI followed 48 h later by D+Q) can maximize clearance of the overlapping senescent pool while allowing immune cells to remove apoptotic debris without overwhelming inflammatory pathways .
In short: FOXO4‑DRI and D+Q do target overlapping senescent cell subsets, especially those that are both p53‑active and BCL‑2‑dependent, and a sequential regimen may exploit this overlap for greater senolytic efficacy.
1 Like
Unless my math skills are eroding, one kit is 10 x 10, or 100 mg, which would cover both of you for $375 a year.
1 Like
I always forget a “kit” is 10 vials, thanks for the correction.
I’d be framing it as 100mg for $375 ![]() a very good price.
a very good price.
1 Like
…or we can try to assemble a group of people interested in customizing HIV-TET linked FOXO4-DRI and try that, like in the studies. I can get it made, but what would a real senolytic hit like that do? I don’t think anyone in the world has tried it.
And no, you don’t get HIV using it. Just needed to add that.
I wouldn’t stick that in me without testing it first, so you can throw in another $400 for Janoshik to check (just) the purity.