I have been fascinated by FOXO4-DRI for a while. The recent 2026 mouse study showed benefits, like to 2017 study. And the 2022 study showed serious harm. Despite the speculative benefits, I have not used it because of the known theoretical risks, and the complete lack of human safety data. I did a deep dive into all the research and as much of the biology as I can understand and I have a link to that research below. I would love any feedback and discussion, either on my notes, or on FOXO4-DRI itself.
FWIW I did a thorough workup on dose and protocol based on all three mouse trials. The mapped dose would be 25 mg intramuscular / day, on alternating days for 5 - 11 total administrations.
It might take 20 years of the age of your critical organs. Or it might make you missing hair start growing again. Or it might not do anything.
And it might cause cancer. Or it might create significant lung damage enough to put you on O2 for the rest of your life. Or it might do nothing.
I have not heard much about this peptide and have not been following it. So, did a quick query on Google Gemini Pro to get a quick overview (not wanting to that long document until I knew a little more):
FOXO4-DRI
Current scientific consensus as of 2026 characterizes FOXO4-DRI (D-Retro-Inverso) as a potent experimental senolytic peptide with robust preclinical evidence but limited clinical validation. Its therapeutic value lies in its ability to selectively induce apoptosis in senescent cells by disrupting the FOXO4-p53 interactome, a mechanism that evades the collateral cytotoxicity often seen with broader senolytics like Navitoclax (Huang et al., 2021).
Mechanism of Action: The FOXO4-p53 Axis
In senescent cells, the transcription factor FOXO4 is upregulated and stabilized via the CHK2-USP37 axis, where the deubiquitinase USP37 prevents its proteasomal degradation (PNAS, 2026). This stabilized FOXO4 binds to the transactivation domain 2 (TAD2) of p53, sequestering it in the nucleus and preventing it from triggering mitochondrial-mediated apoptosis (Frontiers, 2025).
FOXO4-DRI acts as a competitive antagonist. By binding to p53, it induces nuclear exclusion, allowing p53 to translocate to the cytoplasm and mitochondria, subsequently activating the p53/BCL-2/Caspase-3 signaling pathway to execute selective apoptosis in senescent populations (Frontiers, 2025; Zhang et al., 2020).
Preclinical Scientific Evidence
Preclinical data across murine and in vitro human models demonstrate multi-organ benefits:
Target System
Observed Physiological Outcome
Key Finding
Vascular
Improved endothelial function
Reduces P16, P21, and γ−H2AX markers in the aorta; enhances vascular elasticity and lowers pulse wave velocity (PWV) (Frontiers, 2025).
Reproductive
Alleviation of hypogonadism
Targets senescent Leydig cells in aged mice, restoring testosterone secretion profiles (Zhang et al., 2020).
Musculoskeletal
Chondrocyte rejuvenation
Selectively removes senescent human chondrocytes in expanded cultures without affecting healthy PDL3 cells (Huang et al., 2021).
Renal
Reduced frailty
Improves healthspan and renal function in DNA-repair deficient (TTD) and chemotherapy-induced senescence models (Docherty et al., 2020).
Clinical Evidence and Current Status (2026)
Despite robust animal data, the clinical translation of FOXO4-DRI remains in its infancy. As of April 2026, the following “clinical” realities must be noted:
Limited Human Trials: While Phase 1/2 exploratory studies have investigated peptide safety and local administration (e.g., intra-articular for osteoarthritis), large-scale Randomized Controlled Trials (RCTs) confirming systemic efficacy in humans are absent (Dove Medical Press, 2025).
Pharmacokinetic Obstacles: The widespread clinical adoption of FOXO4-DRI is hindered by typical peptide-based limitations: rapid enzymatic degradation, low membrane permeability, and the requirement for injectable administration (PNAS, 2026).
Safety Profile: Preclinical studies suggest high specificity, but the potential for “overkill” in tissues where transient senescence is required for wound healing or tumor suppression remains a point of scholarly debate (Rabinovitch, 2023).
Knowledge Gaps and Scholarly Debates
USP37 as an Alternative Target: Recent discovery of the CHK2-USP37-FOXO4 stability axis suggests that small-molecule inhibitors of USP37 (e.g., Dacarbazine) may offer a more pharmacologically “drug-like” route to achieving the same senolytic effect as the FOXO4-DRI peptide (PNAS, 2026).
Delivery Systems: Current research is shifting toward advanced delivery vectors (e.g., lipid nanoparticles) to overcome the peptide’s inherent instability.
Long-term Toxicity: Data on the impact of chronic, systemic senescent cell clearance on tissue regenerative capacity (stem cell niches) is insufficient.
Expert Summary: FOXO4-DRI is a “surgical” senolytic with a well-defined molecular target, making it superior in theory to broader-spectrum agents. However, until human pharmacokinetic and systemic safety data are published, its use remains restricted to the experimental and preclinical domains.
PNAS. (2026). CHK2-USP37 axis stabilizes FOXO4 to sustain senescence and evade apoptosis. Proceedings of the National Academy of Sciences. https://doi.org/10.1073/pnas.2526252123
FWIW, I do not think FOXO4-DRI has been used in ANY human trials, not Phase 1, not Phase 2, not observational cohorts. Of cuorse, I could be wrong. I’d actually love to be wrong. Can you go back to gemini and ask it about that. I tried and couldn’t find any. I checked ClinicalTrials.gov and no foxo4-dri trials are registered.
I will add “low membrane permeability” was achieved by fusing an HIV-TAT peptide (or HIV-TAT sequence) to facilitate membrane transport and enhance cellular uptake.
I’ve edited this and a couple messages regarding the HIV-TAT sequence. It is included in the F410 product available online.
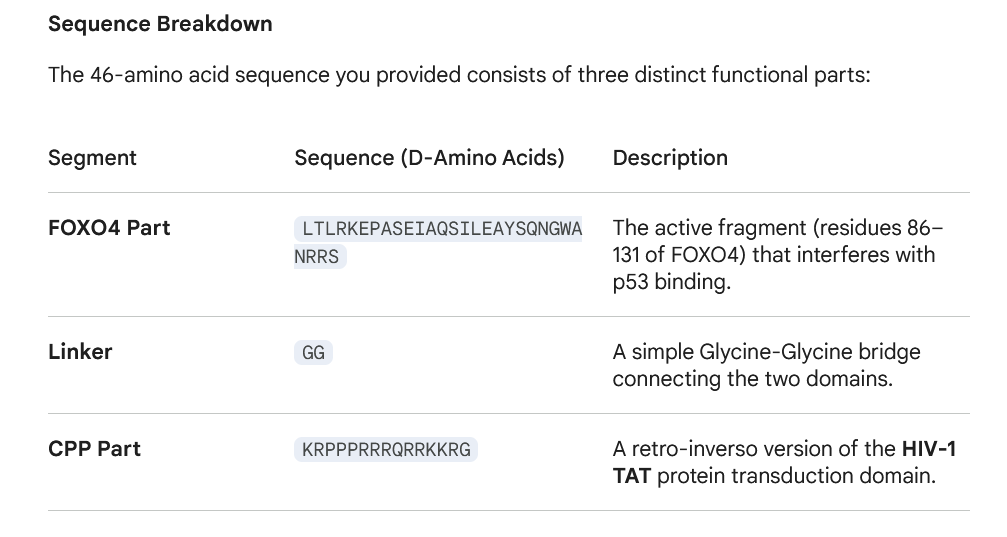
All the studies using FOXO4-DRI used some for of cell transport. They created the peptide as a single amino acid. It is very likely that the peptide being sold by gray vendors is that peptide too and already includes the transport. We just need to verify the exact amino acid chain being constructed. A TAT fusion will include the TAT motif (e.g., YGRKKRRQRRR) or another CPP sequence.
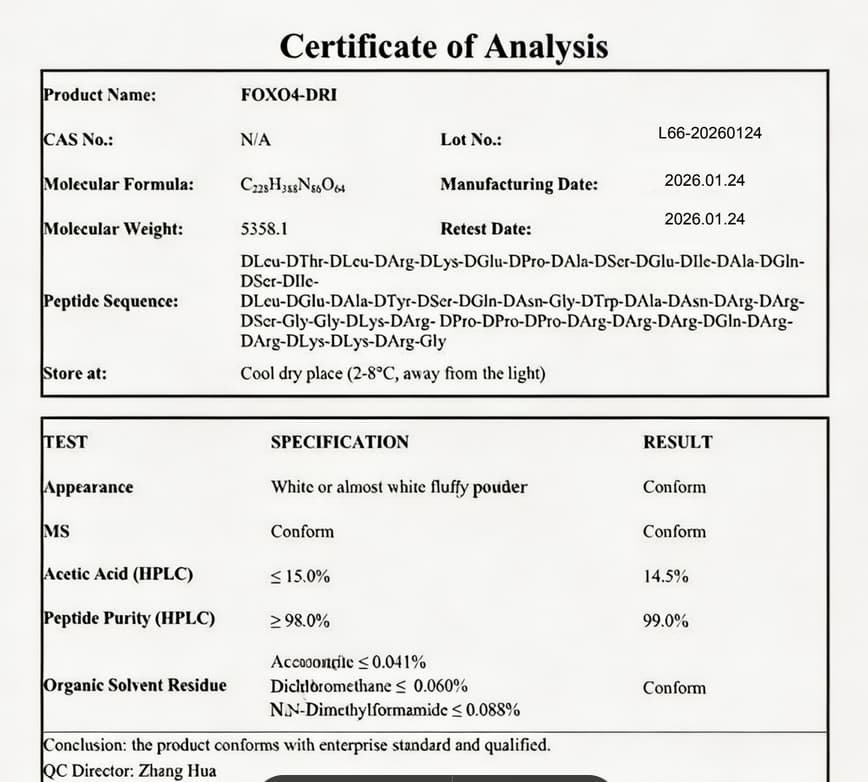
FOXO4-DRI is a D-retro-inverso peptide, meaning its amino acid sequence is reversed and all chiral centers are inverted (L-amino acids are replaced with D-amino acids) to resist enzymatic degradation. The full sequence of FOXO4-DRI is:
100% agree that is just the FOXO4-DRI payload without the CPP tail. It is essentially worthless.
Do we have any reason to believe any gray market vendors made the full amino acid with the CPP?
Do we know what the testing companies are testing against?
If this is really all that is available, then any results people claim are placebo.
I am retracting my agreement, LOL. I did a deeper dive on this sequence.
In sequence terms, that C‑terminal block is exactly the kind of motif that enables membrane penetration,
High local positive charge density Arginine is the key driver — the guanidinium group forms bidentate hydrogen bonds with phosphate and sulfate groups on the cell surface (heparan sulfate proteoglycans, phospholipid headgroups).
Arginine > Lysine for uptake The guanidinium group enables membrane translocation via counterion displacement, something lysine cannot do as effectively.
Flexible, disordered structure Gly‑Gly and Pro‑Pro‑Pro create a non‑helical, adaptable conformation, which is exactly what CPPs use to “thread” through or induce transient defects in the membrane.
All‑D chirality This makes the CPP tail protease‑resistant, which dramatically improves its functional half‑life in biological environments.
What this tail actuallydoesin practice
Initial binding to the cell surface via electrostatic interactions
Internalization through a mixture of:
direct translocation (rare but possible with strong poly‑Arg motifs)
endocytosis (the dominant route for most CPPs)
Partial endosomal escape Poly‑Arg motifs can destabilize endosomal membranes, but escape efficiency varies widely.
This CPP‑like tail is expected to significantly enhance cellular uptake of the peptide.
This is the 46‑residue D‑retro‑inverso FOXO4‑derived peptide used throughout the in‑vitro and in‑vivo experiments in the paper and it is an exact match for the COA you uploaded.
If the substance you get from gray tests as a match for the uploaded COA it is exactly what was injected into mice in the Bear paper.
To be clear, if I was going to run this experiment on myself, I would absolutely do third party testing on a sample vial after my purchase.
It’s not that expensive gray. $650 buys enough for a full treatment of 150 mg, and spend another $400 for testing one vial.
And according to the original research paper from Bear 2017, and Janoshik testing, and the COA you upload and I verified with one of my gray suppliers, it is exactly the same identical molecule used in the original mouse studies.
But the discussion I want to have is, would you use it? How would you decide to use it?
This is a treatment with a very real biological mechanisms that may kill you… END YOUR LIFE. and we don’t know if that is a 1% chance or 0.0001% chance. Or a 10% chance. No idea.
And it may rejuvenate your organs and increase your health span. It may make hair grow again on your bald spot or reverse your gray hair. There are biological mechanistic reasons for all of the above. Or it may do nothing. No idea.
How should anyone interested in health and longevity make such a decision.
I’m really healthy for my age. Should I just keep going the gym, eating well, and take my proven supplements?
Is it just greed to want more when more comes with such risks?
“I’m really healthy for my age. Should I just keep going the gym, eating well, and take my proven supplements?”
I would say yes, stick with the proven longevity treatments you have listed. Without any real human data, you would be rolling the dice with this peptide (or any research peptide), no matter how fascinating the scientifc evidence may be to you.
Again, how would any of you know it’s working? Given the data I’ve shown that it should not cross the cell membrane. D&Q on the other hand has been shown to work…
Have you tried D&Q&F or do you feel that Q/F is too similar? Maybe D&F instead?
Also @researcher6076, have you used D&Q combination? I can attest that dasatib is available from the known sources and is relatively less expensive than Chinese FOXO4-DRI. I will go update the info on the other forum as wel.
yes I expect looking for the senolytic markers via blood work would be a specific ordeal. I’ve also read from others that they get flu-like symptoms. How long did it last for?
Wouldn’t it make more sense to extend telomeres before cell division is required?
yes, I also have a protocol I’m following atm. I’m avoiding the peptides you mentioned there though due to their angiogenic properties, and nad, idk, seems like nicotinic acid maybe the best overall choice, given the latest research talk.
But Epitalon I tried at 1mg for 10 days. I’ve read of others using 10mg for 10 days. I may increase the next cycle. It didn’t disrupt my sleep, and something in my stack (I think maybe reta) has fixed my waking/sleep cycle for the better… mostly. Sometimes I wake up too early, and that never happened before, but I’m also on newer bp meds, so maybe that’s why. How much epitalon were you using?
I’ve not done the senolytics before except for quercetin use over some time now. I’ve been pulsing it now over the last couple months, 1200 mg but just on tues,wed,thurs. AI seems strigent on that course. I received some Dasatinib just today and have some Fisetin as well. I was planning on trying this week…