A hypothalamic neuropeptide called orexin drives the small, unconscious movements that burn surprising amounts of calories, and this system fades with age, potentially explaining why activity drops and weight creeps up across the lifespan.
Some people fidget. They pace on phone calls, jiggle their legs, stand rather than sit, and reorganize the kitchen for no reason. Others sit still. That difference, it turns out, is not just personality, it is neurochemistry, and it may be one of the most underrated levers in metabolic health.
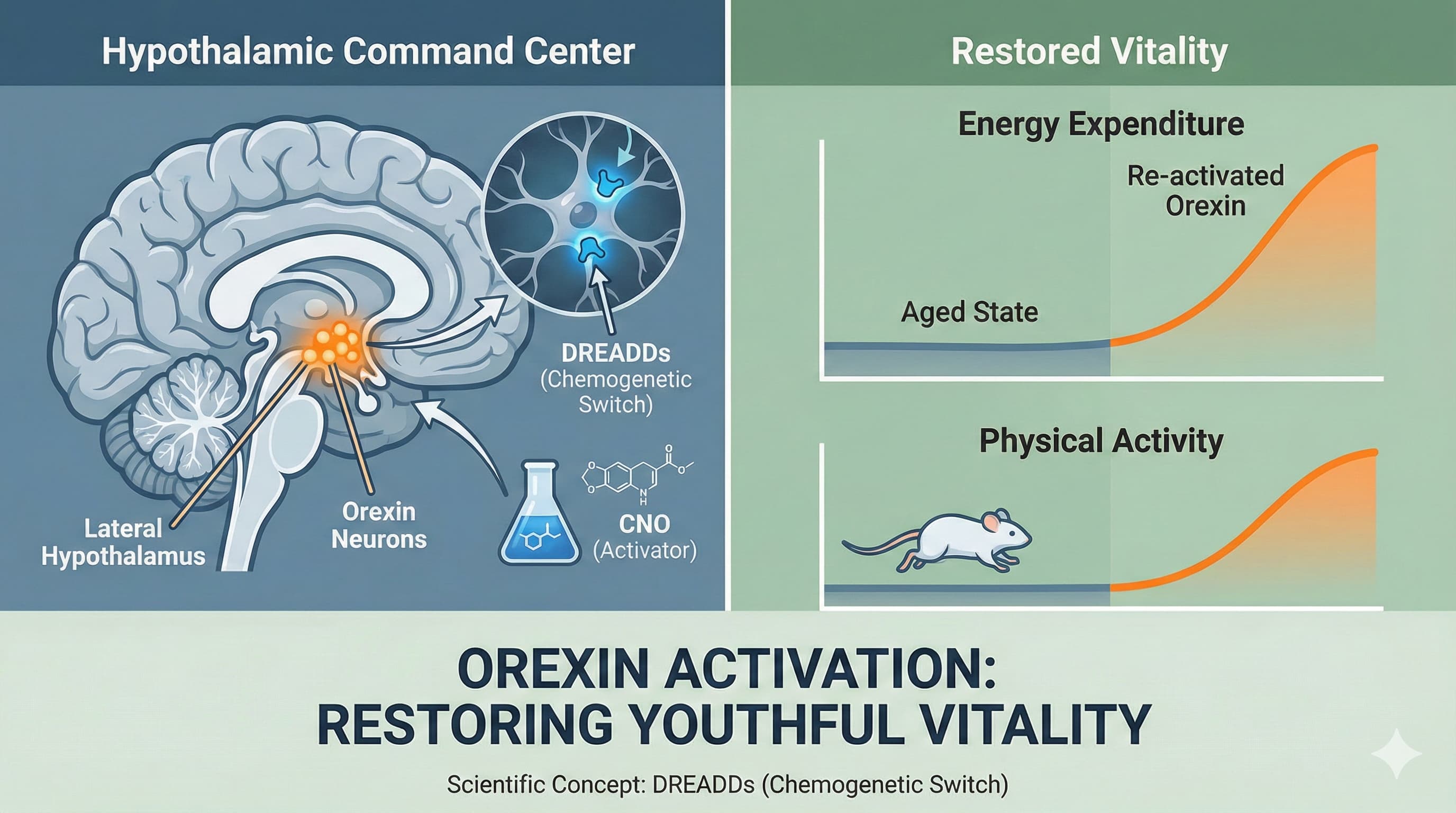
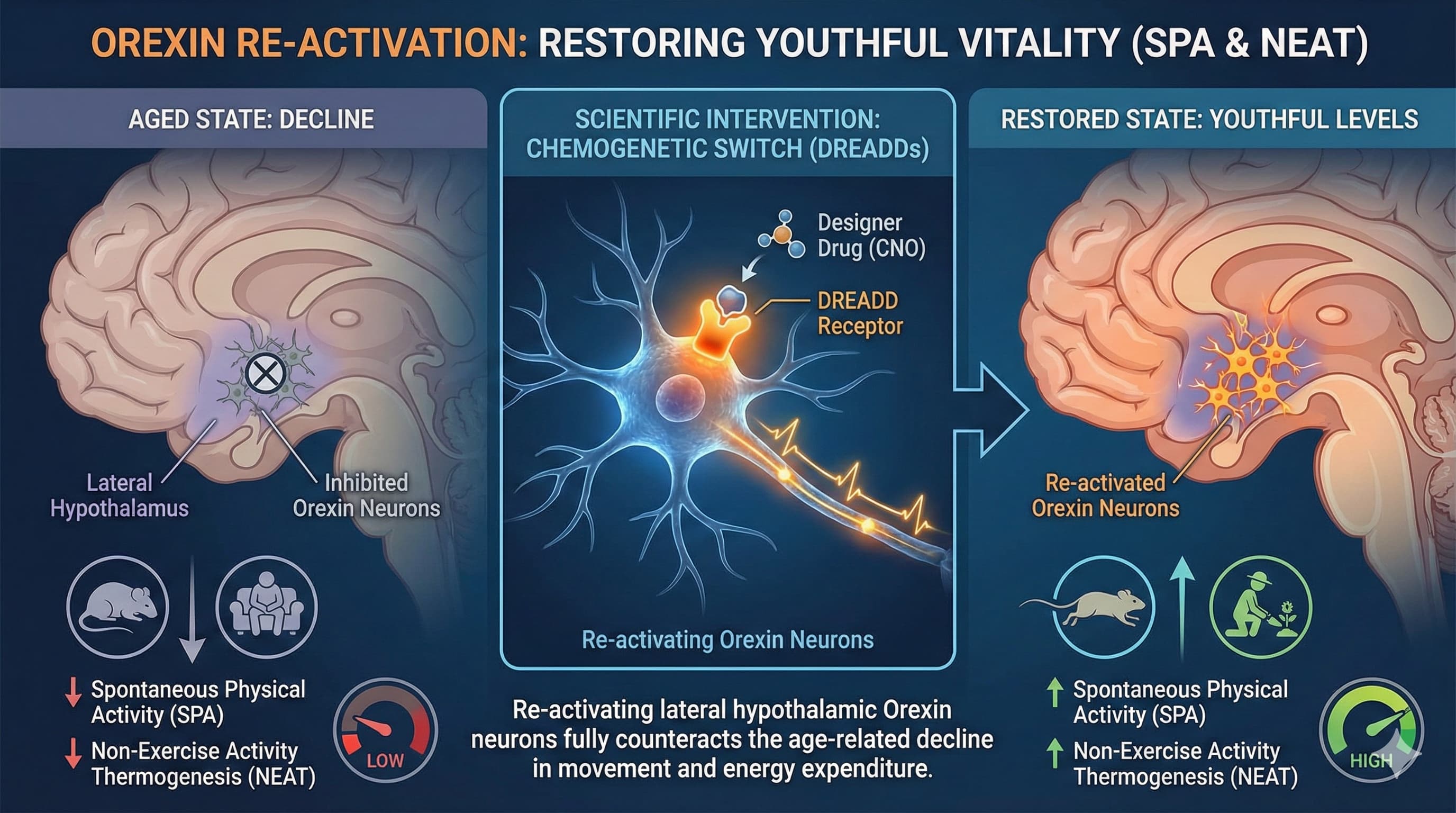
This 2014 review from the University of Minnesota and the Minneapolis VA pulls together a decade of work on orexin (also called hypocretin), a neuropeptide made by a small cluster of neurons in the hypothalamus. Orexin is famous for one thing: when these neurons die, you get narcolepsy. But the same cells do something quieter and arguably more important for longevity. They drive what researchers call spontaneous physical activity, or SPA, and the calories it burns, nonexercise activity thermogenesis, or NEAT.
The big idea is that NEAT is not trivial. The authors cite work showing that lean people spend roughly 150 extra minutes per day on their feet compared to obese people, a difference large enough to matter for body weight over a lifetime. And orexin appears to be the upstream signal that sets this dial. Inject orexin A into the right part of a rat’s hypothalamus and it starts moving more within minutes. Animals with naturally high orexin signaling resist becoming obese even when fed a high-fat diet, without eating less.
Here is the longevity hook. Orexin signaling does not stay constant. It rises through development, peaks in adulthood, and then declines with age. As orexin drops, so does spontaneous movement, and so does the body’s ability to defend a healthy weight and a stable circadian rhythm. The same decline is loosely linked to the cognitive and sleep problems that accumulate in old age, and to the dramatic orexin neuron loss seen in Parkinson’s and Alzheimer’s brains at autopsy.
The provocative implication, which the authors are careful to frame as a future direction rather than a finished result, is that age-related weight gain, daytime sleepiness, and reduced activity might share a common upstream cause: a quietly failing orexin system. If true, drugs that selectively boost orexin tone could one day target the “I just don’t feel like moving” problem directly, rather than relying on will power to exercise.
Actionable Insights
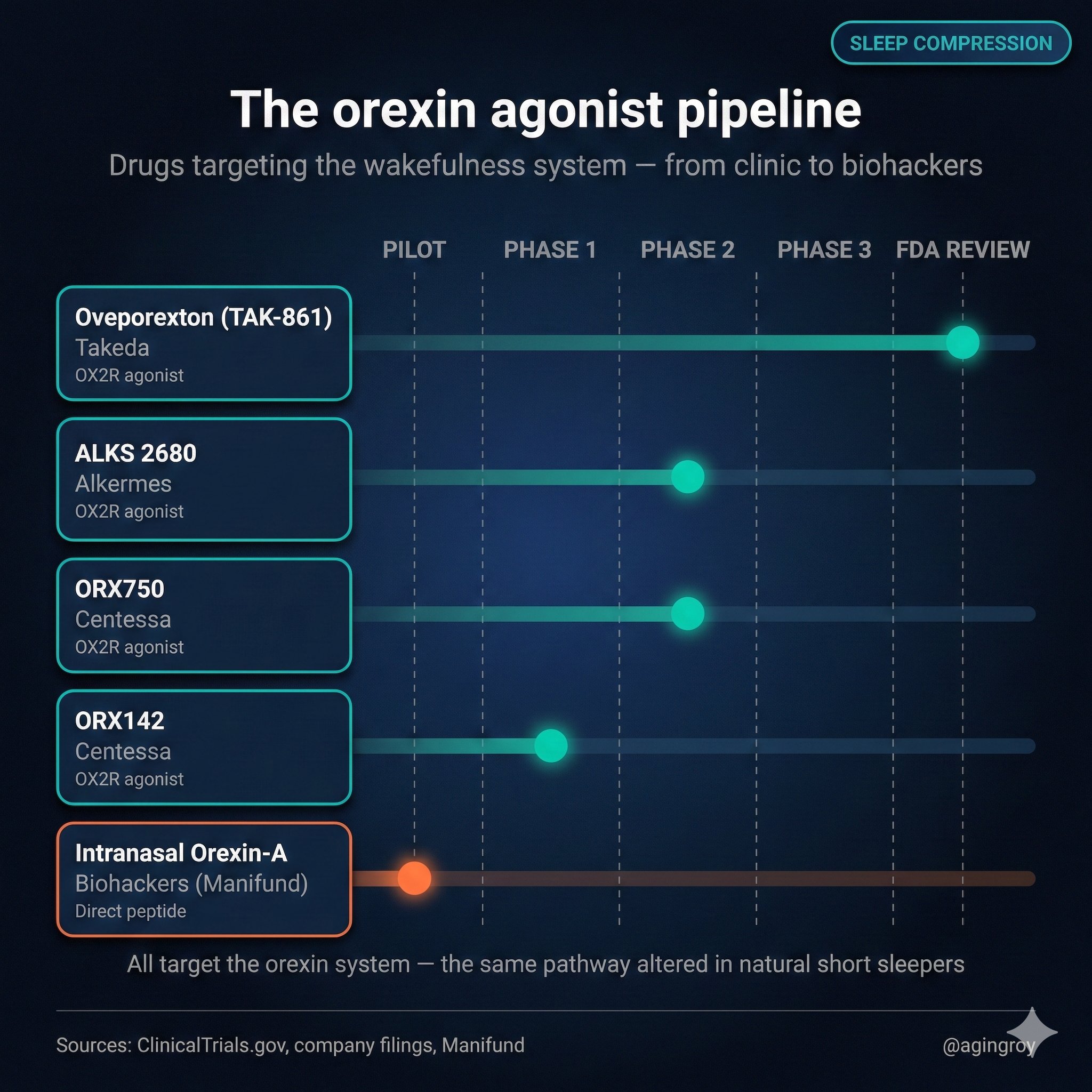
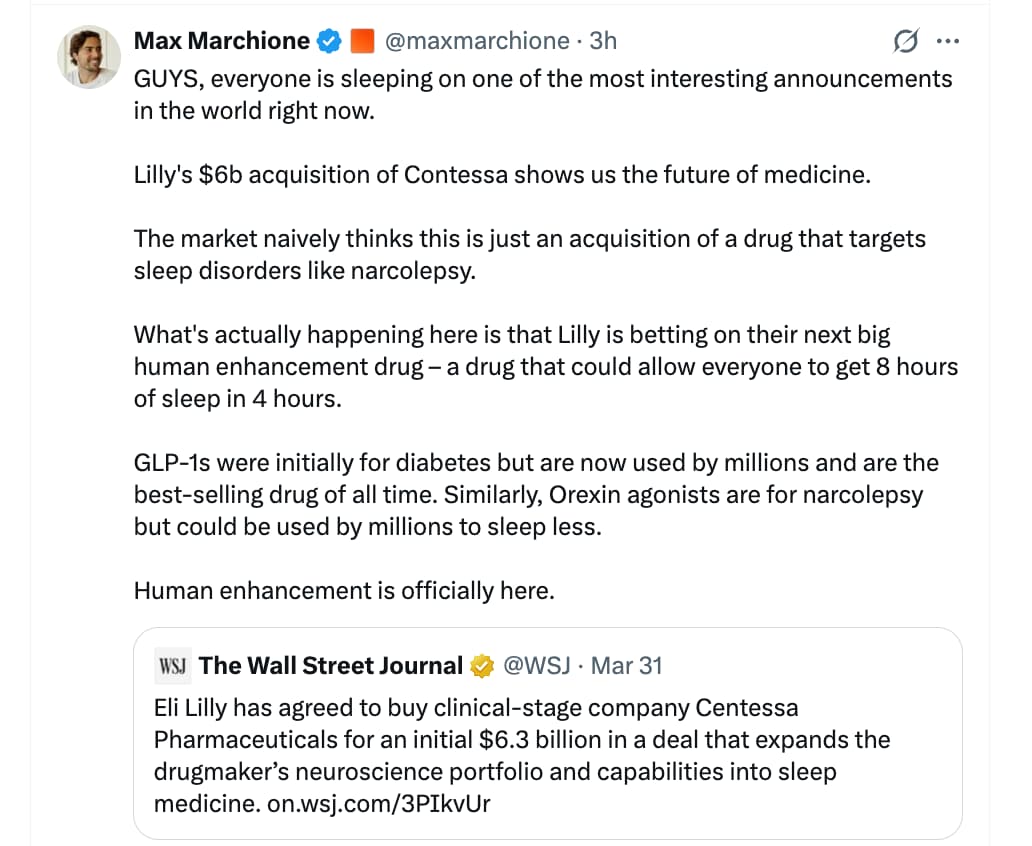
The honest answer is that this paper offers no validated human intervention yet. While new drugs are in phase 3 clinical trials and one is scheduled to be released by the end of 2026, there is currently no orexin pill you can take. But two extractable, real-world signals are worth stating with their effect sizes.
First, the NEAT effect is large in absolute terms. The cited human data show lean individuals accumulate about 150 extra minutes of daily movement and sit roughly 2 hours less than obese individuals, translating to an estimated additional 5 kcal/kg/day of energy expenditure. For an 80 kg person that is roughly 400 kcal/day, on the order of a daily training session, achieved entirely through posture and ambulation rather than structured exercise. The take-home: standing, pacing, and low-intensity movement are not metabolically trivial, and deliberately increasing them is the closest current proxy for “boosting orexin-driven activity.”
Second, the directionality matters for behavior. In animals, high baseline activity precedes and protects against weight gain rather than merely following from leanness. This supports front-loading movement habits before metabolic decline sets in rather than after.
Source:
- Open Access Paper: Zink et al., The orexin neuropeptide system: physical activity and hypothalamic function throughout the aging process,.
- Institution: University of Minnesota & Minneapolis VA Healthcare System, USA.
- Journal: Frontiers in Systems Neuroscience
- Impact Evaluation: The impact score of this journal is ~3.5 (Impact Factor), evaluated against a typical high-end range of 0–60+ (e.g., Nature), therefore this is a Medium impact journal. It is a reputable specialty journal but relies heavily on synthesizing pre-clinical data rather than breaking large-scale human trials.