Hidden in a plate of shiitake mushrooms is a molecule that may be quietly keeping your cells alive. Ergothioneine (ET) — a sulfur-rich amino acid first isolated from ergot fungus in 1909 — has spent over a century in relative obscurity. That may be about to change.
A sweeping new systematic review published in Ageing Research Reviews synthesizes 20 years of evidence (2005–2025) and makes a forceful case: ET is not merely an antioxidant curiosity but a plausible geroprotector — a compound capable of targeting multiple molecular mechanisms that drive biological aging simultaneously.
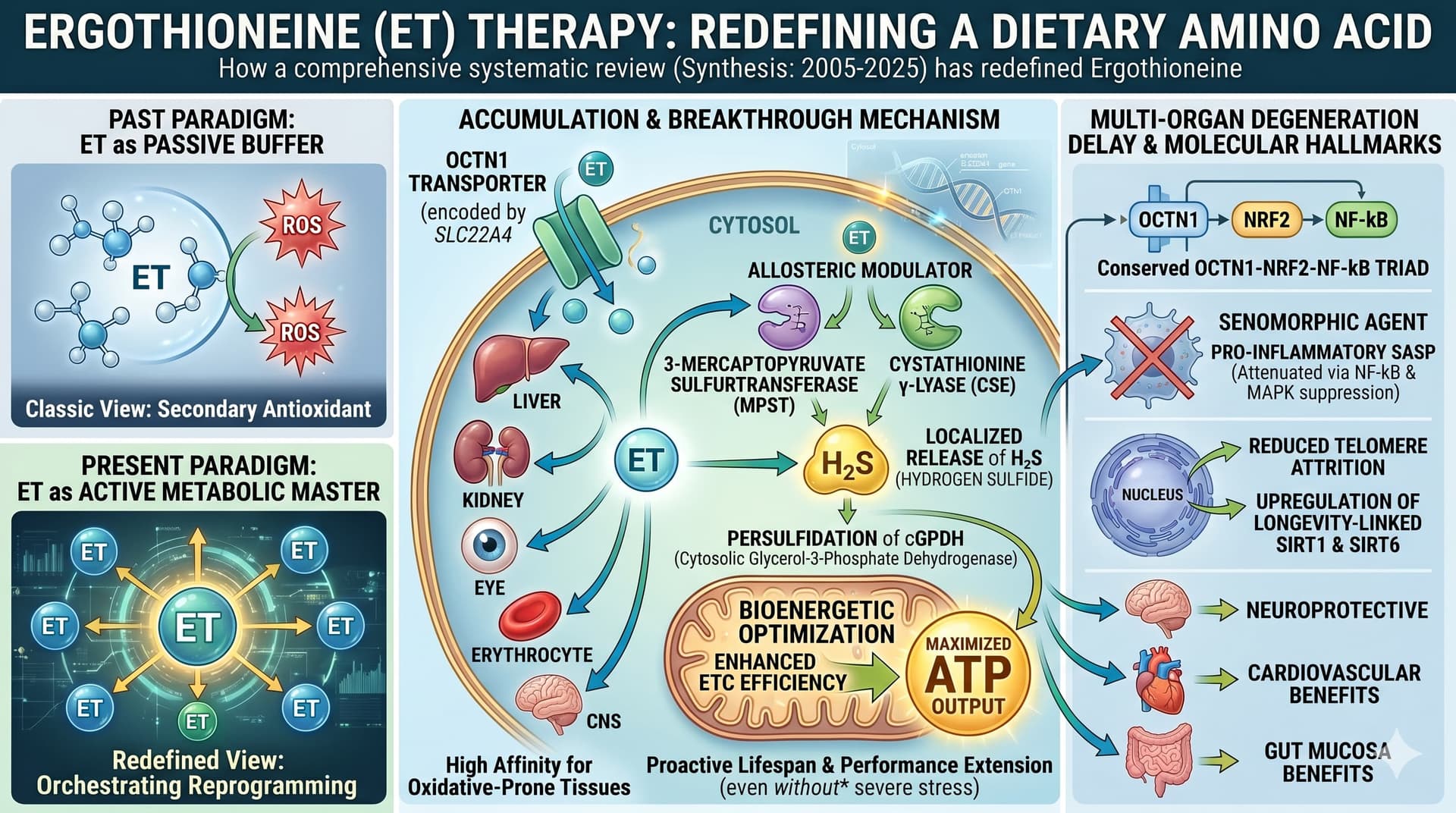
The big idea begins with a specialized protein called OCTN1, encoded by the gene SLC22A4. Unlike generic antioxidants that spray-and-pray across tissues, OCTN1 acts as a precision delivery system, ferrying ET specifically into the cells and organs most vulnerable to oxidative damage: the brain, liver, kidneys, eyes, and bone marrow. This selective accumulation is not passive — it is active, energy-dependent, and regulated. Critically, blood levels of ET peak in adolescence at approximately 3.7 mg/100 mL and then decline progressively with age. Lower ET levels have been independently correlated with frailty, mild cognitive impairment, Parkinson’s disease, and all-cause mortality in large cohort studies. This age-related depletion pattern is one reason Nobel laureate biochemist Bruce Ames proposed the “longevity vitamin” hypothesis — the idea that ET is a micronutrient we chronically under-consume, and whose deficit accelerates aging.
The review maps ET’s effects onto the canonical “Hallmarks of Aging” framework. Its actions span telomere preservation (by protecting guanine-rich telomeric DNA from oxidative attack and upregulating SIRT1/SIRT6), mitochondrial quality control (restoring mitophagic flux via PINK1/Parkin pathways), suppression of the pro-inflammatory Senescence-Associated Secretory Phenotype (SASP) via NF-kB inhibition, and modulation of the mTORC1-S6K1 nutrient-sensing axis.
But the most intellectually disruptive finding reviewed here concerns a newly characterized mechanism: ET does not merely neutralize reactive oxygen species — it actively reprograms cellular energy metabolism. Recent data from two independent 2025 studies (Petrovic et al. and Sprenger et al.) demonstrate that intracellular ET binds and activates key sulfur-trafficking enzymes (MPST and CSE), triggering localized hydrogen sulfide (H2S) production. This H2S then persulfidates cytosolic glycerol-3-phosphate dehydrogenase (cGPDH), directly enhancing electron transport chain efficiency and maximizing ATP output. This elevates ET from “defensive scavenger” to “proactive metabolic optimizer” — a mechanistic upgrade with profound implications.
In male mice, ET supplementation at 4–5 mg/kg/day extended median lifespan by 16% and mean lifespan by 21% (Katsube et al., 2024). In Drosophila, lifespan extension was demonstrated across multiple dose ranges.
The honest caveat: human RCT data remains thin. A large cohort study of 3,236 participants over 21 years shows compelling observational links between plasma ET and reduced cardiovascular mortality, but causality is not established. Phase 1 and Phase 2 human trials confirm safety up to 25 mg/day with no adverse signals, but adequately powered, long-term efficacy trials with hard clinical endpoints do not yet exist.
Actionable Insights
The most immediate practical signal from this review is dietary: eat mushrooms. Oyster, shiitake, and king oyster mushrooms contain 1–7 mg ET per gram dry weight, making them by far the richest accessible source. Regular mushroom consumption is the primary way to counter the age-related decline in blood ET levels.
Second, genetic context matters. If you carry the SLC22A4 L503F (C1672T) variant, standard dietary intake may be insufficient to raise tissue ET to protective levels — and counterintuitively, this variant may increase autoimmune risk in inflammatory contexts. Genetic testing for SLC22A4/SLC22A15 polymorphisms could eventually guide individualized ET protocols.
Third, ET operates as an “on-demand” protector: supplementation in healthy, low-stress individuals produces minimal biomarker changes. The benefit signal strengthens under oxidative load — which means individuals with metabolic syndrome, cardiovascular disease, neurodegenerative risk, CKD, or those undergoing hemodialysis (where ET is depleted by 88%) represent the clearest candidates for supplementation trials.
Pulsed Dose: ET exhibits non-linear pharmacokinetics, high systemic accumulation, active renal reabsorption, and an exceptionally long human half-life of approximately 30 days. Continuous daily high-dose supplementation risks saturating the limited capacity of the OCTN1 transporter and may impede the absorption of essential physiological cations or co-administered drugs like metformin. Intermittent pulse dosing is theoretically superior to avoid transport bottlenecks.
Mandate Baseline Genetic and Microbiome Screening: Supplemental ET is highly context-dependent and presents an unexpected biological “Achilles’ heel”. Certain anaerobic gut bacteria express ET hydrolases that cleave ET into trimethylamine (TMA), which the liver converts into trimethylamine-N-oxide (TMAO)—a notorious pro-atherogenic metabolite linked to accelerated vascular aging and cardiovascular disease. Individuals must profile their gut microbiome and verify their SLC22A4 genotype (specifically checking for the L503F variant, which dramatically alters baseline transport efficiency) before initiating heavy, unmonitored supplementation protocols.
The current clinically validated dosage range is 5–25 mg/day, with safety confirmed up to 16 weeks in elderly subjects.
Source:
- Paywalled Paper: Ergothioneine as a potential geroprotector: Targeting molecular hallmarks of ageing and age-related diseases
- Institution: Department of Pharmacology (School of Pharmacy) and Department of Radiology (Shengjing Hospital), China Medical University, Shenyang, China.
- Journal Name: Ageing Research Reviews.
- Impact Evaluation: The impact score (CiteScore) of this journal is 13.1 (based on standard index data for Ageing Research Reviews),therefore this is a High impact journal.