There are some interesting indication where combination of interventions are done and more of that will come in future.
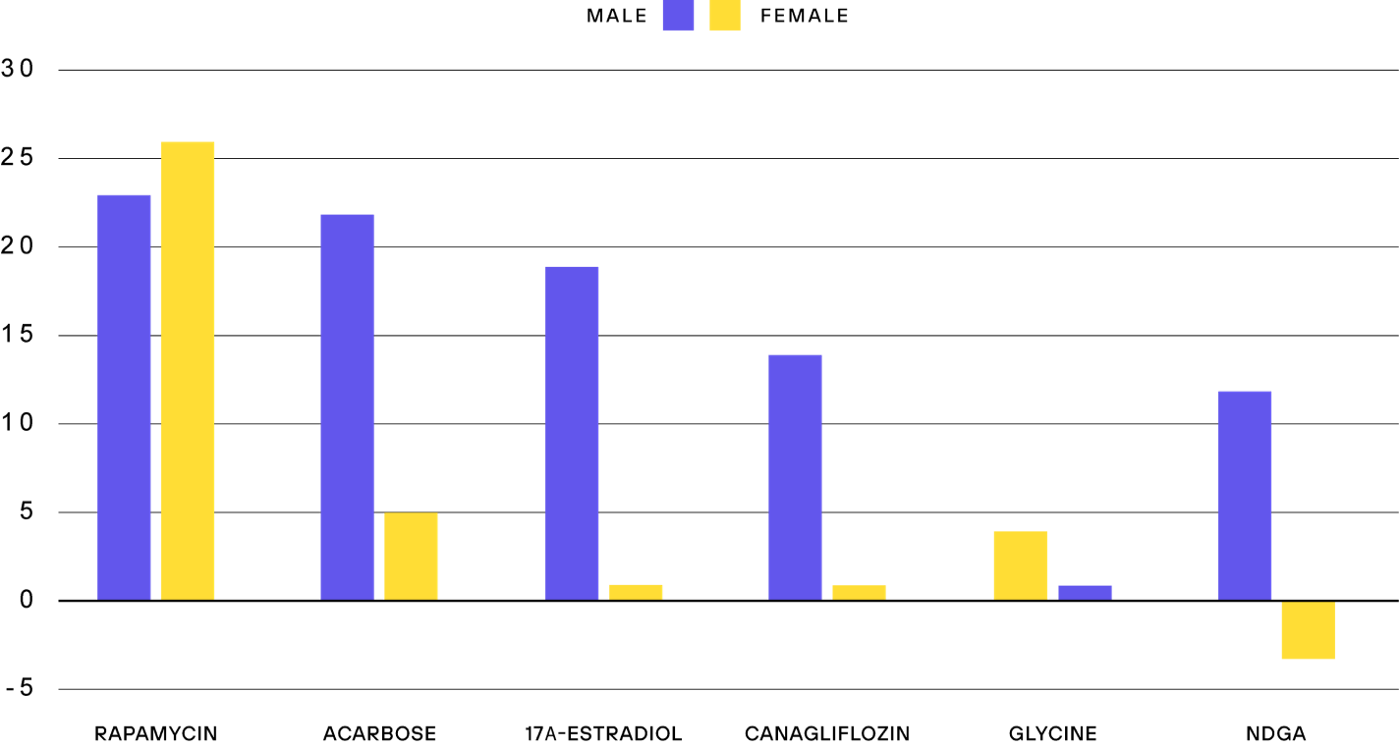
Here is for example a combination with rapamycin and acarbose in the ITP which lead to the biggest increase male lifespan which they have reported.
Here is interesting additative effects when rapamycin is combined with calorie restriction.
Here is one study on the additative effect on rapa and CR on fruit flies:
Even if these are interesting indications of promising combinations between interventions we are long from getting everything optimal. I really like this image that I created awhile ago to point out that it’s all about finding the right balance between anabolism and catabolism.
Possibly acarbose should be separated from SGLT2 inhibitors and both items listed. They act upon the body in very different ways and I think (please any forum members correct me if I am wrong) they both have beneficial effects apart from carbohydrate restriction effects.
Regarding cost of rapamycin I think three plus is too low price. There are many people here trying to lower their cost of rapamycin and some people don’t have the money for buying it. Here in Sweden if I buy it from the pharmacy the cost is 386 USD for 100 mg so my yearly cost will be around 1100 USD depending on dose. It’s quite much money if you compare that to calorie restriction which is free and even saves money. But let’s see what the other two interventions cost. Do you know what the yearly cost of Acarbose is?
That is a really great price! Is that common in the USA? Then I understand @DeStrider why you want more plusses on rapamycin. Is it the same price for you?
I purchase mine from India and use GFJ, so my cost is about 3 USD per week. That would be 156 USD per year. Even less if I take a month washout period every so often. So costs vary wildly between locations.
I am very interested in 17A-Estradiol. It works on a different pathway than Rapamycin, correct? I am hoping for a larger add-on effect. Any idea when it may be commercially available?
I also am hoping for a larger add-on effect. We are perhaps 3 to 5 years away from it becoming commercially available as a unique drug; the only company I’ve heard of that is doing anything with it is Apollo ventures, and one of our forum members mentioned here that they are still just doing animal trials - so its a long way away from FDA approval.
That said, its just the other version of Estradiol that is already used by millions of women (beta-estradiol), and my understanding that given that in any manufacturing process of estradiol there will likely be both versions of this chiral molecule included in the ultimate product, so women are already taking it in their regular hormone treatment. Of course, the “alpha” version of the molecule hasn’t been trialed in men yet, so formal clinical trials still need to be done.
Yes - I looked at NDGA. It looked interesting, but it was pulled from the market many years ago due to human toxicity issues.
Sleep is obviously important to staying healthy, just like breathing is. But I don’t think I’ve ever seen a scientific study that shows that that you can increase longevity with sleep.
Good sleep keeps you alive longer because you’ll die without it, just like you’d have a miserable, short life if you didn’t eat and breath properly. But you’re not going to add years to your life through sleep.
I feel like a few people in this forum are confusing “you’d be unhealthy without this” and “you’ll increase your natural lifespan with this.”
I have heard of Alpha-ketoglutarate in different podcast but I have seen lifespan data on it yet. Thanks for the studies. My guess is that this compound is not in a place to be classied as the best intervention we have. But it would probably be a compound to have in another list. Let’s call that list for example “Upcoming longevity future compounds to keep an extra eye on”
Very interesting point! But the science that a combination strategy I would say is not that strong yet. More studies needs to be done on this before it can be qualified to be best intervention. Now it’s only ITP which has shown this which is great but it would be even better to see it replicated in different species. Safety profile etc. There is lots of unknown factors here. But very promising combo!
Ah, great helpful diagram! Peter Attia did suggested that Canogliflozin would be probably better at place third instead of Acarbose. What do you think about that?
Yes, 17A-estradiol is a interesting one! Curious, what pathways are we taking about when it comes to 17A-estradiol which differs from rapamycin? Because biological processes have a tendency to go into each other.
Interesting response from Peter. Lifespan increase larger in acarbose but yes more good additional health data on canagliflozin. I defer to Peter on all things medical.