First of all - I think your view is the dominant view of many of those in the medical profession who are at all familiar with rapamycin (if they are at all supportive of people taking rapamycin), and given the nascent state of the rapamycin clinical trials for aging that may be entirely appropriate.
Also - Its absolutely true that Mtor is critical during growth - so you don’t want to experiment with rapamycin until you stop growing. I’m not a biologist - so I will deign to their expertise if they want to weigh in on this, but all that I’ve read suggests that most if not all human development is complete by age 25 to 27. For example this article talks about 25 for the completion of brain development.
I have a cardiologist friend who says the only thing that keeps growing after that are your nose and your ears - and thats why they seem so large on old people. Perhaps the lack of infinite growth of the nose and ears would be another benefit of taking rapamycin I haven’t mentioned 
I agree there are lingering concerns about the risks of inhibiting mTOR in people of reproduction age and that rapamycin use / mTOR inhibition is definitely not recommended (and the risk, of course, is that someone is taking Rapamycin and doesn’t realize they are pregnant) - so definitely extra caution is required during those age periods.
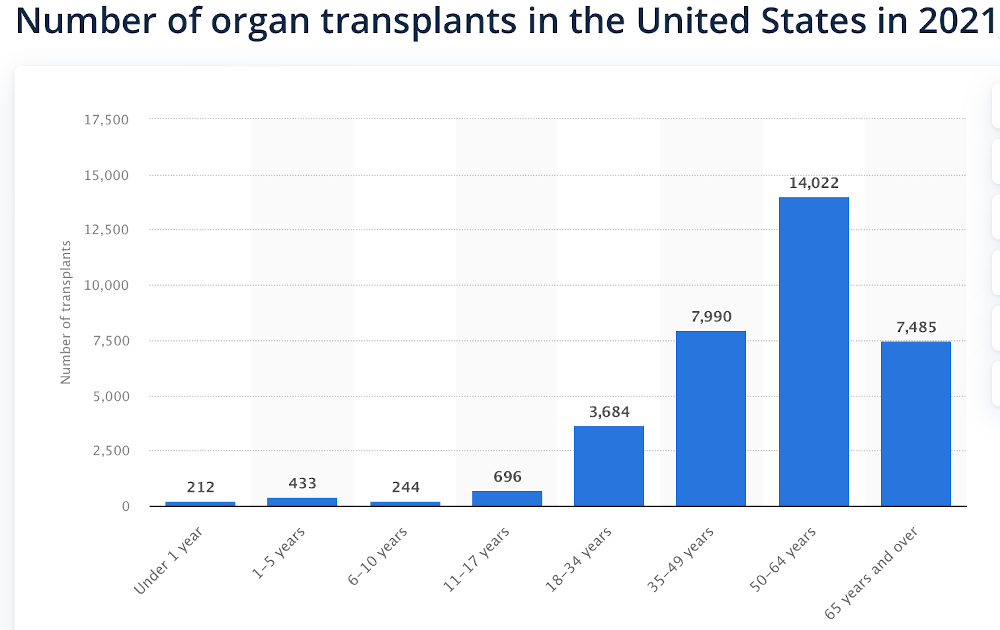
But - I would argue that given that perhaps something like 25% of organ transplants happen to patients under the age of 40 (see graph below), and virtually all of these patients probably take sirolimus (I believe taking it with cyclosporine is the typical medication protocol used in transplant patients), and I suspect that most of these people also go on to have children (or at least a significant portion). So - I would argue that the medical profession has been dealing with the risk of mTOR inhibition and potential pregnancy for the past 20+ years with rapamycin (as long as rapamycin has been used in this application) and there is not that much difference with it going forward in an anti-aging application with people of this age group. But yes, the anti-aging doctors would need to learn about this and implement these educational programs in their clinics if they treat this age group.
Also - you are correct I think that the typical healthy 30 year old is not going to see much benefit immediately from taking rapamycin in terms of inflammation reduction, etc. and still needs mTOR to grow.
But - we all need mTOR for our muscles to grow, we just don’t need mTOR on all the time for our muscles to grow, and rapamycin for anti-aging protocols are all about periodic dosing, to allow mTOR to return to higher levels periodically to help in muscle growth, etc. when its needed. So - a 30 year old would get that on the periodic dosing schedule just as a 60 year old would too.
Maybe there are a number of factors that will ultimately evolve to drive the medical profession’s thinking on this, and consumer’s thinking.
-
Current concerns with fertility. This is a common concern of professional women in their late 20s and early 30s who place a high priority on their careers. One strategy they pursue right now is freezing their eggs, but that is an expensive, painful and risky medical process too. While still to be proven, rapamycin may simplify this process. I suspect most women of this age would prefer to take rapamycin at a cost $50 a month or so, than the $6,000 to $20,000 for egg freezing - and all that that entails.
-
Concern about, and Risk of, Obesity (and how well the research on rapamycin in preventing obesity is progressing). The sooner you can stop the problem of obesity, the better. This is definitely one area where a large percentage of people are still growing during their 30s and 40s - but would probably prefer to not be growing.
-
Risk / Reward Perception - the science around rapamycin is changing every year, and people all have different risk/reward perceptions and profiles. So I think you’ll see the adoption rate of rapamycin vary as research progresses and the risk / reward profile of taking rapamycin becomes better understood by people.