In a significant shift from its reputation as merely a reproductive hormone or a bodybuilding drug, a new major review in Nature Metabolism (Institution: Harvard Medical School & Tulane University, USA) redefines testosterone (T) as a critical “metabolic messenger.” Authored by heavyweights Franck Mauvais-Jarvis and Shalender Bhasin, this paper argues that T is essential for systemic homeostasis, regulating glucose, lipids, and energy balance across multiple organs.
The “Big Idea” here is the integration of T into the longevity pharmacopoeia not for lifespan extension per se, but for healthspan preservation. The authors dismantle the outdated view of T as purely “anabolic/androgenic,” highlighting its dual mechanism: it signals directly through the Androgen Receptor (AR) and indirectly via conversion to 17β-estradiol (E2) acting on Estrogen Receptors (ER). This “crosstalk” is vital for insulin sensitivity in muscle, lipolysis in adipose tissue, and beta-cell function.
Crucially, the paper leverages data from the landmark TRAVERSE trial to quell fears regarding cardiovascular (CV) toxicity, arguing that maintaining physiologic T levels in hypogonadal men is metabolically protective. However, for the longevity biohacker, the distinction is critical: while T fixes metabolic “broken parts” (hypogonadism, insulin resistance), it has not been proven to extend maximum lifespan in rigorous wild-type animal models, unlike its metabolite 17α-estradiol.
Source:
- Open Access Paper: Metabolic Messengers: testosterone
- Impact Evaluation: The impact score of Nature Metabolism is 20.8, evaluated against a typical high-end range of 0–60+ for top general science, therefore this is an Elite impact journal.
Part 2: The Biohacker Analysis
Study Design Specifications:
- Type: Review / Perspective (Synthesizes data from Preclinical Models and Clinical Trials, including the TRAVERSE study).
- Subjects: N/A (Review). Discusses C57BL/6J mice and Humans (Hypogonadal Men).
Mechanistic Deep Dive:
-
The Dual-Pathway: T is a “pro-hormone.”
- AR Signaling: Increases muscle mass (glucose sink) and reduces visceral fat (lipolysis).
- Aromatization to E2: Essential for vascular health and preventing fat accumulation. Blocking conversion (via Aromatase Inhibitors) negates many of T’s metabolic benefits.
-
Organ Priorities:
- Muscle: Enhances mitochondrial biogenesis and insulin signaling.
- Liver: Suppresses steatosis (fatty liver).
- Pancreas: Protects β-cells from glucotoxicity (via AR).
Novelty: This paper formally codifies the shift from “T for libido” to “T for metabolic syndrome.” It integrates the TRAVERSE trial safety data to argue that T therapy is a viable tool for reversing pre-diabetic phenotypes in men, provided hematocrit is managed.
Critical Limitations:
- Translational Gap: The benefits in hypogonadal men (restoring deficiency) do not prove efficacy in eugonadalmen (supra-physiological biohacking).
- The Neutrophil Problem: A concurrent 2025 study (e.g., Nature Communications, Svedlund Eriksson et al.) suggests T exacerbates cardiac injury after acute myocardial infarction by increasing neutrophil infiltration. This contradicts the “cardioprotective” narrative in the acute setting.
- Missing Data: Long-term data on T’s effect on aging rates (methylation clocks) is absent.
Part 3: Claims & Verification
Claim 1: “Testosterone therapy improves insulin sensitivity and glycemic control in men.”
- Verification: Confirmed. Meta-analyses show T reduces fasting glucose and HbA1c in hypogonadal men with Type 2 Diabetes.
- Hierarchy: Level A (Meta-analysis of RCTs).
- Source: Diabetes Care Meta-Analysis
Claim 2: “Testosterone is safe for the cardiovascular system (MACE events).”
- Verification: “Safe” is relative. The TRAVERSE trial showed non-inferiority (did not cause more heart attacks than placebo) in a high-risk population. However, it did increase rates of atrial fibrillation and pulmonary embolism.
- Hierarchy: Level B (Large Scale RCT - TRAVERSE).
- Confidence: [Medium - Specific risks exist].
Claim 3: “Testosterone reduces visceral adiposity.”
- Verification: Strongly supported. T stimulates lipolysis and inhibits triglyceride uptake in adipocytes via AR.
- Hierarchy: Level A/B.
Claim 4: “Testosterone extends lifespan.”
- Verification: FALSE / UNPROVEN in wild-type organisms. It improves healthspan in disease states (hypogonadism), but fails ITP lifespan tests.
- Hierarchy: Level D (Animal Data - Negative Result in ITP).
Part 4: Actionable Intelligence
The Translational Protocol (Rigorous Extrapolation):
-
Human Equivalent Dose (HED):
- Note: Do not use animal conversion for T; use established clinical TRT dosing.
- Standard TRT: 100mg Testosterone Cypionate per week (IM/SubQ).
- HED Math (for reference): A mouse dose of 10mg/kg/week ≈ 0.81 mg/kg human dose. For a 75kg male, this is ~60mg/week. (Clinical doses are often higher to overcome SHBG binding).
-
Pharmacokinetics (PK/PD):
- Bioavailability: Oral T is useless (liver destruction). Must be Injectable, Transdermal, or Pellet.
- Half-life: Cypionate/Enanthate esters have a half-life of ~8 days. Weekly or twice-weekly dosing is required to prevent “troughs” that trigger mood instability.
-
Safety & Toxicity Check:
- Erythrocytosis (Thick Blood): T stimulates erythropoietin (EPO). TRAVERSE trial confirmed significant increases in hematocrit. Action: Phlebotomy if Hematocrit > 54%.
- Prostate: Does not cause cancer, but will accelerate growth of existing androgen-dependent tumors.
- Liver: Injectable/Transdermal bypasses the liver (unlike oral 17-alkylated androgens).
- Cardiovascular: WARNING: Avoid if recent MI (<6 months). Recent 2025 data suggests T worsens neutrophil-mediated damage post-MI.
-
Biomarker Verification Panel:
- Efficacy: Free Testosterone (calc), SHBG, HbA1c (target <5.0%), Fasting Insulin (target <5 uIU/mL).
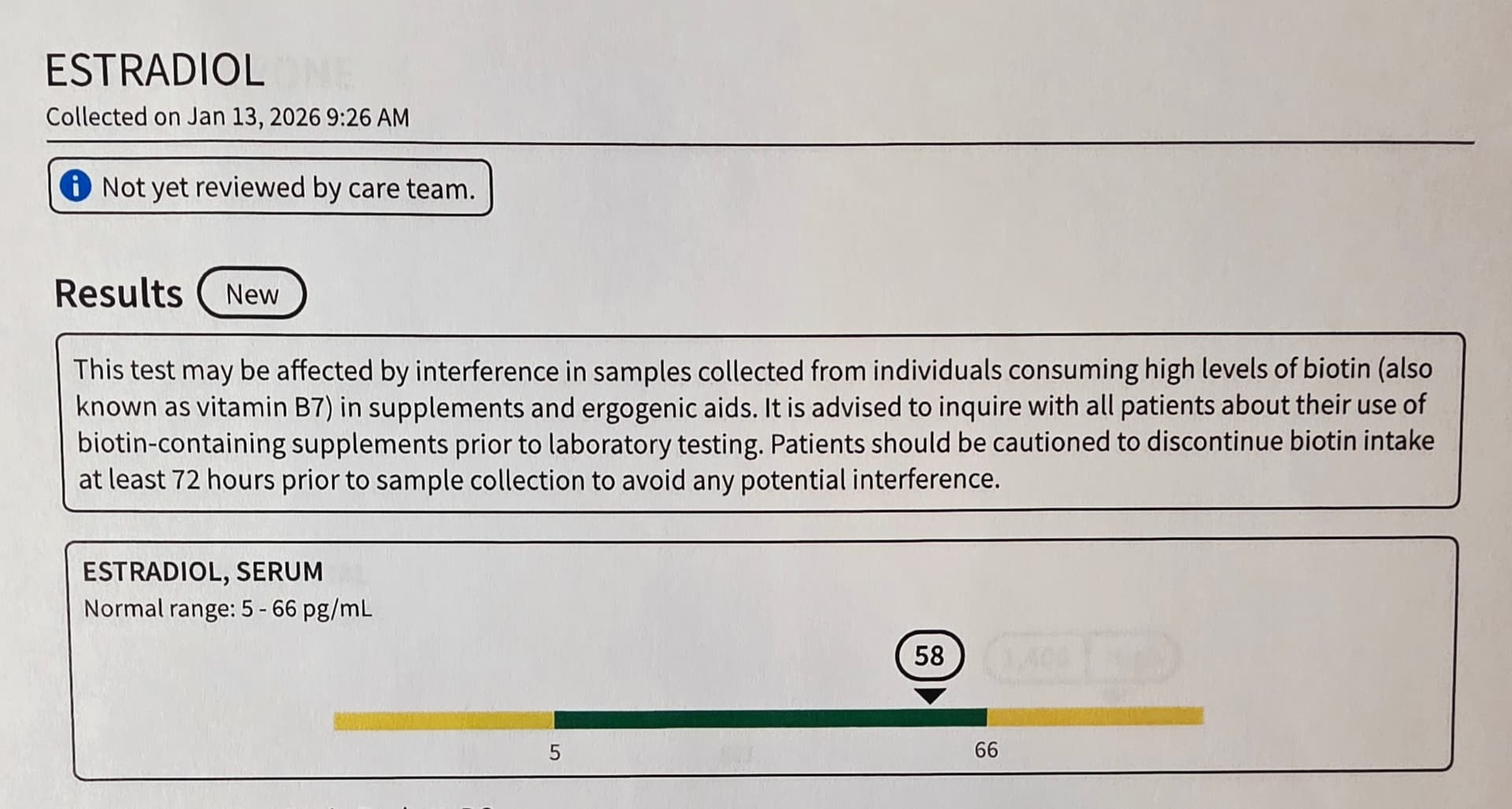
- Safety: CBC (Hematocrit), PSA (Prostate), Estradiol (sensitive LC/MS), Lipid Panel (T may lower HDL).
-
Feasibility & ROI:
- Cost: Generic T-Cypionate is Cheap (~$20/month).
- ROI: High for quality of life/body composition. Low/Null for absolute lifespan extension.
Part 5: The Strategic FAQ
- Q: Does Testosterone actually extend life, or just make the engine run hotter?
- A: Likely the latter. It is pro-growth (mTOR). Longevity generally favors maintenance (autophagy) over growth. T improves quality (healthspan) but likely trades off against maximum duration (lifespan).
- Q: How does this interact with Rapamycin?
- A: Potentially Synergistic. Rapamycin inhibits mTORC1 (longevity), while T stimulates mTOR (muscle). Cycling them or using them together might allow “anabolic maintenance”—keeping muscle mass while preserving autophagy.
- Q: Should I block the conversion to Estrogen (use an AI)?
- A: NO. The review emphasizes that T’s metabolic benefits (insulin sensitivity, vascular health) rely partly on aromatization to Estradiol. Crashing E2 ruins the metabolic ROI.
- Q: Is there a conflict with Metformin?
- A: Potential blunting. Metformin can blunt the exercise-induced mitochondrial adaptations that T supports. However, for pure glycemic control, they are additive.
- Q: Why did the ITP find 17α-estradiol extends life but Testosterone doesn’t?
- A: 17α-E2 improves glucose tolerance and lowers inflammation without the anabolic/androgenic load of T. It suggests the “feminizing” (or at least non-androgenic) pathway is the pro-longevity one.
- Q: Does T therapy mimic the “Neutrophilia” risk seen in the recent MI study?
- A: Possibly. The mechanism (CXCL12 downregulation in bone marrow) appears intrinsic to Androgen Receptor activation. If you have a heart attack while on T, the damage might be worse.
- Q: What is the “Sweet Spot” for trough levels?
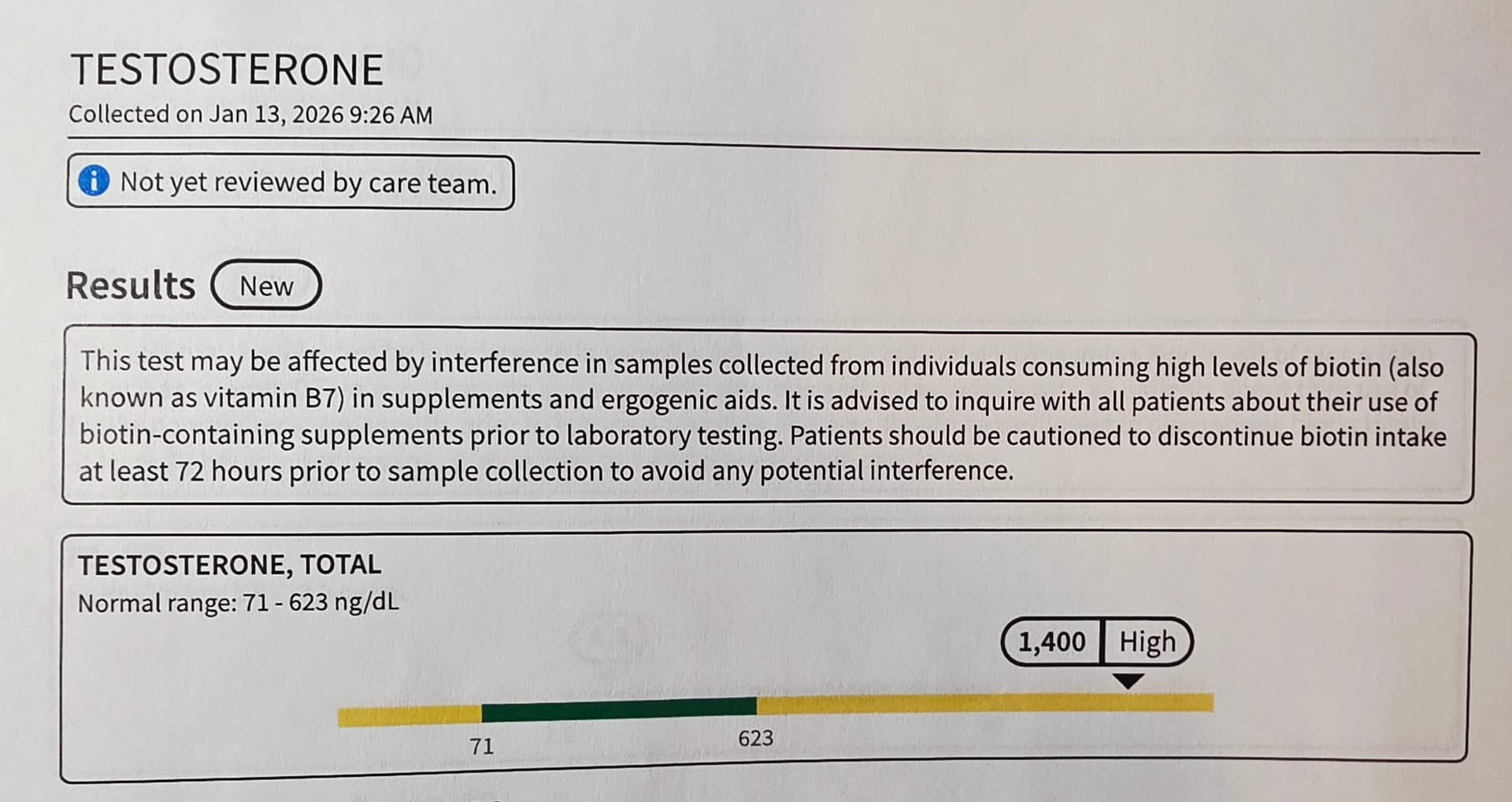
- A: [Confidence: High] aim for the upper quartile of “youthful” normal (e.g., 700–900 ng/dL Total, 15–25 ng/dL Free). Supraphysiological levels (>1500 ng/dL) dramatically increase hematocrit/CV risk.
- Q: Can women use this “Metabolic Messenger”?
- A: Yes, but dosing is critical (1/10th male dose). T is essential for female metabolic health, muscle, and bone density, though often ignored.
- Q: Does T worsen Sleep Apnea?
- A: Yes. It is a known side effect. Hypoxia from apnea + T-induced erythrocytosis is a dangerous stroke cocktail.
- Q: Is this “Biohacking” or just “Medicine”?
- A: For hypogonadal men, it’s medicine. For eugonadal men seeking optimization, it’s biohacking with real risks (infertility, dependency). The review supports the medical correction of metabolic syndrome via T.