I had similar procedure in Russia long ago without sedation. In the U.S. it’s not possible - I tried. They don’t offer even TNE (trance nasal endoscopy) with thinner scope. Clinics are set up for sedated procedures — staffing, scheduling, and recovery rooms are built around it. That’s why it so expensive!
1 Like
Actually, I never thought about it. They just did it as part of the procedure. They used:
Twilight anesthesia, formally known as conscious sedation or Monitored Anesthesia Care (MAC), is a technique that uses mild doses of drugs to induce a state of deep relaxation and temporary memory loss while allowing you to remain conscious."
Unlike general anesthesia, you are not fully “put under”; you can typically breathe on your own, respond to verbal cues, and follow simple instructions during the procedure."
I have had this 4 times, once for a hernia repair, once for cataract surgery, and twice for colonscopies. I like it. It felt pleasant to me and had no side effects (that I know of).
It was odd in the effect that on two of these occasions, I asked when we were going to start, and the procedure had already happened.
2 Likes
Did you have to ask for it or you were offered MAC?
No, I really didn’t ask. As these were pretty routine procedures, I just followed instructions.
1 Like
These days MAC is propofol. I was completely out, unconscious, but I could breathe on my own. It was fun-- a lovely high.
Then they took me off it, high wore off in a few hours, but feeling of being drugged didn’t until 28 hours had passed.
1 Like
I’ve done most of mine without anesthesia, but the last one I did with because the doctor wouldn’t let me do it without and I didn’t want to bother to find a new doctor!
1 Like
Yeah, and this one has a lot of history and massive studies in the UK
Anyone on the forum ever do or look into?
Medtronic’s PillCam COLON 2 (colon capsule endoscopy) - a non-invasive, data-rich option
It aligns well with a mission of proactive, high-definition health optimization: it provides direct visualization of the colon (without sedation or radiation) and can serve as a practical “first-pass” assessment for patients who want to go beyond stool-based tests—helping determine whether a traditional colonoscopy is truly necessary for biopsy or polyp removal.
While PillCam COLON 2 is FDA-cleared for specific indications in the U.S., this “triage/filter” approach has already been deployed at scale in the UK, including NHS pathways and evaluations involving over 10,000 patients, and the broader PillCam platform has been used in millions of procedures worldwide.
See e.g.
1 Like
Different kind of cancer, but just shows we should never ignore discomfort …which I’m guilty of doing.
4 Likes
Yeah, ovarian cancer is a nasty one because there’s no screening test, there are few symptoms at the early stages, and from what I understand it’s even fairly difficult to diagnose based on things like ultrasound which you might have routinely for other reasons.
3 Likes
On the subject of colon cancer I just posted a new thread that has a very strong correlation with this I Found the Philosopher’s Stone! Death begins in the colon - and so we must not ignore it!
Dried Plums Drive Gut Microbiome Shifts but Fail to Halt Colon Carcinogenesis in Rats
The relationship between dietary fiber, gut microbiota, and colorectal cancer (CRC) prevention remains a highly debated topic in nutritional oncology. A recent in vivo study investigated whether the consumption of prunes (dried plums)—a food rich in fermentable fibers, sorbitol, and polyphenols—could mitigate tumor development in a chemically induced colon cancer model. Over a 32-week feeding trial, male Wistar rats were administered weekly injections of the carcinogen 1,2-dimethylhydrazine and fed either a matched basal diet, a 5% prune diet, or a 10% prune diet.
The primary hypothesis was that the highly fermentable components of prunes would increase the production of short-chain fatty acids (SCFAs), specifically butyrate, thereby reducing colonic tumorigenesis. While the prune-supplemented diets did indeed radically alter the gut microbiome and significantly elevate total cecal SCFAs and butyrate levels, these physiological changes failed to reduce the incidence, count, or volume of colonic tumors.
Notably, the data revealed a non-significant trend toward fewer small intestinal tumors in the prune-fed cohorts, suggesting that the protective effects of fermentable fibers like pectin may be highly localized. Furthermore, the prune diets decreased epididymal fat pad weights without altering total caloric intake, pointing toward an uncoupled metabolic benefit likely driven by intestinal viscosity. Ultimately, this data challenges the prevailing assumption that merely elevating colonic butyrate via dietary fermentation is sufficient to yield chemopreventive effects against CRC, highlighting a critical knowledge gap in our understanding of microbiome-metabolite-host interactions.
Context
- Open Access Paper: Prune (dried plum) consumption does not reduce colonic tumor formation but drives beneficial changes in the gut microbiome of rats
- Institution: University of Minnesota, St. Paul, MN.
- Country: United States.
-
Journal: Food & Function (Royal Society of Chemistry).
Impact Evaluation The impact score of this journal is approximately 5.4, evaluated against a typical high-end range of 0–60+ for top general science, therefore this is a Medium impact journal.
Part 2: The Biohacker Analysis
Study Design Specifications
- Type: In vivo (chemically induced carcinogenesis model).
- Subjects: Male Wistar rats.
- Total N: 81.
-
Cohorts: * Basal Control: n=29.
- 5% Prune Diet: n=25.
- 10% Prune Diet: n=24 (tumor analysis) / n=21 (metabolite analysis).
Mechanistic Deep Dive
-
Epigenetic Regulation via Butyrate: Butyrate is an established histone deacetylase (HDAC) inhibitor, a mechanism widely speculated to confer chemoprotection by preventing the epigenetic silencing of tumor suppressor genes. This study successfully achieved a linear, dose-dependent increase in cecal butyrate via prune supplementation. However, the failure of this elevated butyrate to attenuate colonic tumors suggests that either the localized concentration was insufficient, or that endogenous fermentation-derived butyrate lacks the chemopreventive efficacy frequently observed in in vitro cell culture models. [Confidence: Medium].
-
Inflammatory Pathways (NF-kB & Wnt/beta-catenin): The researchers investigated colonic mucosal markers, specifically looking for suppression of the pro-inflammatory transcription factor NF-kB and the Wnt-pathway regulator beta-catenin. Prune consumption yielded no significant modulation of these proteins, nor did it reduce systemic calprotectin.
-
Organ-Specific Aging Priorities (Metabolic Tissue): Interestingly, the 5% prune cohort exhibited significantly reduced liver and epididymal fat pad weights despite identical caloric intake and terminal body weights. This indicates a potential modulation of lipid metabolism and adiposity, likely mediated by the soluble fiber (pectin) content altering nutrient absorption kinetics.
Novelty This paper isolates the limits of dietary prebiotics in cancer prevention. It demonstrates that driving beneficial shifts in the microbiome—such as increasing the abundance of Lachnospiraceae (Blautia , Coprococcus ) and the archaeon Methanosphaera —does not automatically translate to halted carcinogenesis. The positive correlation between Methanosphaera and total SCFA production is a highly novel finding, warranting further investigation into the role of archaea in human longevity and metabolic health.
Critical Limitations
-
Translational Uncertainty: 1,2-dimethylhydrazine is a potent, synthetic DNA-alkylating agent. While it reliably produces tumors, it bypasses the chronic, low-grade inflammatory etiology that drives most spontaneous human colorectal cancers. [Confidence: High].
-
Absence of Inflammatory Baseline: The control diet did not mimic a standard “Western Diet” (i.e., it was not high-fat or high-sugar). The lack of baseline inflammation likely masked any potential anti-inflammatory properties of the prune polyphenols, rendering the NF-kB data inconclusive.
-
Confounding Variables in Diet Design: The basal diet utilized non-fermentable cellulose as its sole fiber source, while the prune diets introduced highly fermentable pectin. Consequently, the study actually measures the difference between fermentable and non-fermentable fibers, rather than isolating the specific polyphenol or micronutrient effects of the prunes themselves.
2 Likes
So many supplements and medicines that are supposed to prevent colon polyps have been a complete failure for me. Maybe they prevented the old style polyps but not the new style.
I think the key here is that there are 2 types of colon cancer - the traditional cancer that develops in older adults and the newer cancer that develops in younger adults. These two types of colon cancer also form in different parts of the colon. The new type develops in the rectum and the side of the colon closest to the rectum. Traditional colon cancer forms in the middle and the side closest to the small intestine.
The only way to definitely prevent both is with a colonoscopy.
3 Likes
This sort of experiment is not very useful IMO. Chemically inducing tumours really doesn’t have any relevance to the way that humans develop cancers.
If you know anything about statistics, this study is MASSIVELY underpowered. They’ve got ~25 rats per group, with the highest tumour incidence of 86%. So in order to actually detect a significant change in tumour formation, with 80% power at a = 0.05… you’d need almost 60 rats per group, not 25. In order to detect a p ≤ 0.05 significant change in tumour incidence, they’d need to see a 60% reduction in tumour formation, which is almost impossible. So a negative result isn’t a surprise, and it doesn’t actually tell us anything about prunes and colon cancer anyway.
Plus, they seem to have a huge number of end points: tumour incidence, count, volume, in multiple locations, fat pad weights, the microbiome, fecal analyses… so basically it’s very likely that they’ll find something significant to talk about, which is exactly what they did with the butyrate etc.
4 Likes
And I can’t imagine eating enough prunes to really make a difference - I have started leaving most of the skin on the green banana I put in my Jade Smoothie (I just peel off the very outer layer) the fibrous peel is strangely satisfying to chew on once blended. That or a plate of cooked and refrigerated lentils or potatoes gives a lot more bulk for your colon to ferment than a few prunes would.
1 Like
I don’t disagree about the colonoscopy but I hadn’t heard about two kinds of tumours? I thought it was pretty clear that most were at the distal end.
No. Based on my research there appears to be two types, early and late onset, but they are usually clumped together as colon cancer. The difference is where and when the polyps appear. Early onset is much more dangerous IMHO due to people waiting to screen until it is too late.
1 Like
This is more “science” than “medicine / translation”, but very interesting:
Naturally Occurring Bacteria Completely Eradicate Tumors in Mice With a Single Dose
In experiments using a mouse model of colorectal cancer, researchers observed an extraordinary outcome after administering E. americana through a single intravenous injection. The treatment completely eliminated tumors in every case, resulting in a 100% complete response (CR) rate. This level of effectiveness was far greater than what is typically seen with established cancer therapies such as immune checkpoint inhibitors (anti-PD-L1 antibody) and the chemotherapy drug liposomal doxorubicin (chemotherapy agent).
4 Likes
A new take on the causes and solutions to the increasing risk in youth of colorectal cancer:
Why are early-onset colorectal cancer rates spiking?
You may have heard that early onset colorectal cancer has doubled in the past 30 years. This claim is true, but undersells the phenomenon - “early onset” is medically defined as “under the age of 50.” If you focus only on colorectal cancer in children (individuals under 18 years of age), there has been a ~400% increase in incidence1.
Why? To some extent the answer to this question is unknowable2, but a wide range of explanations have been proposed, from obesity to microplastics to dietary changes. Many of these influence colorectal cancer risk by affecting the microbiome, shifting it away from an enrichment of symbiotic bacteria and towards a higher ratio of aggressive, pro-inflammatory microbes.
But how does changing the microbiome cause cancer? The answer, in many cases, is very direct.

Read the full story: Why are early-onset colorectal cancer rates spiking?
Related:
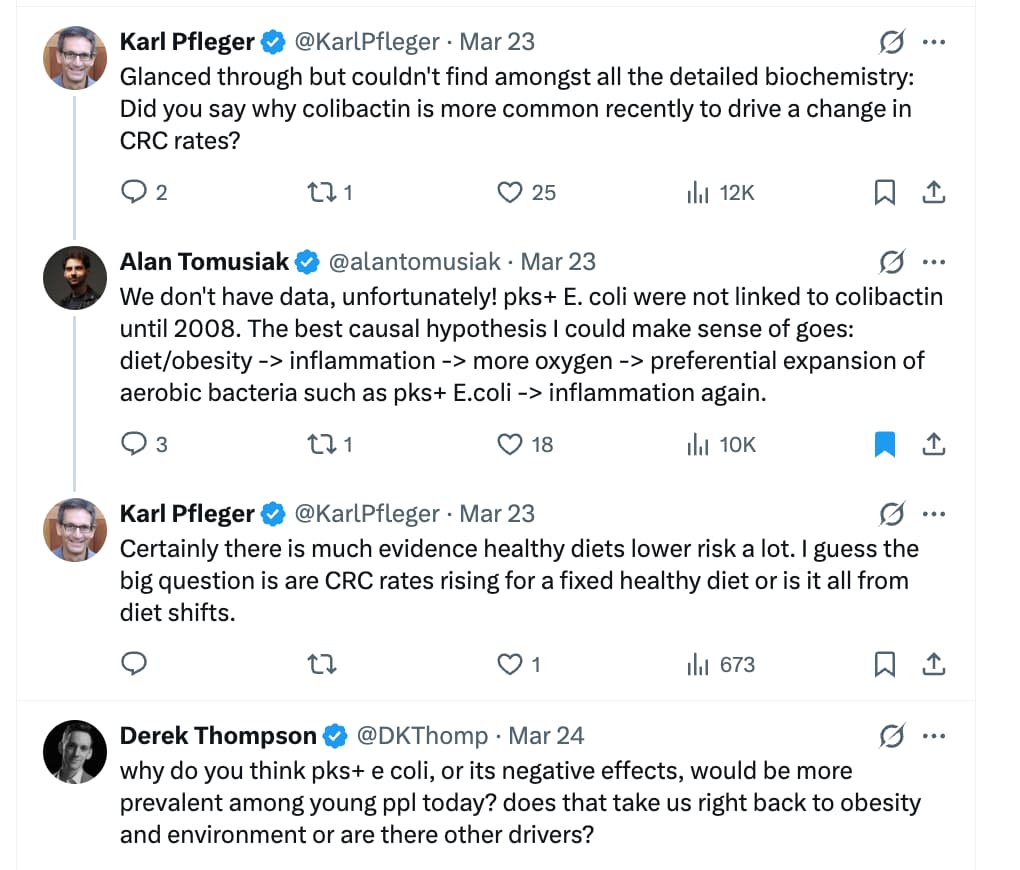
Source: https://x.com/alantomusiak/status/2036138383584665964?s=20
1 Like
Young colon cancer linked to specific fats in ultra-processed foods
A few new clues are emerging.
At the annual American Society of Clinical Oncology conference in Chicago this week, several presenters coalesced around the idea that young-onset colorectal cancer is a distinct disease from the kind that tends to hit people in their late 60s or early 70s.
Too much oil and grease, not enough nuts and fish
Dr. Ning Jin at The Ohio State University has gone straight to the source to better understand young colon cancer. She’s investigated a small set of 16 tumors from young-onset colorectal cancer patients and compared them to 26 older patients’ tumors. Her work has pinpointed 11 cancer genes that are more prevalent in young people, revealing what she calls a new genetic “fingerprint” for young colon cancer.
“Our study showed that early-onset colorectal cancer is a biologically unique disease,” Jin told Business Insider. “The cancer behaves differently.”
4 Likes
Even when polyps are removed during colonoscopy, your risk of CRC may remain elevated for a decade or more. This could be due to the microbiome.
Long-lasting gut microbiome and fecal metabolome alterations after colorectal adenoma removal and their relationship to colorectal cancer
https://www.cell.com/cell-host-microbe/fulltext/S1931-3128(26)00177-0
Pop-sci article:
Gut changes linger years after polyp removal and may signal colorectal cancer risk
5 Likes