I will note that this approach is true if they are definitively palliative/terminal - not much surprise there with a lot of patients seeing an oncologist. There are plenty of older folks who are considered polypharmacy and not even close.
I will also note my dad who used to manage a CAR-T therapy trial had patients (trial participants) who were told to do that by their oncologist - until the trial showed ~90% remission rates and severely messed with the previous oncologist’s Kaplan Meier curve determinations. Not every oncologist is close to aware of all the possible experimental approaches, let alone an accurate prediction of what those approaches may yield. A prediction on what cell based/gene based therapies have a shot often becomes too complex for a human expert-only approach - there’s a reason why the former Genentech CEO went to Calico to get access to cutting-edge computational biochemistry approaches with the best possible tools.
Oncologists also tend to believe in giving up on what they believe is terminal (not everyone of course) and I found if I don’t ask an expert about experimental approaches I’ve already researched well with PhD researchers in the field - I don’t get any options (I appeared to have controlled pathological myopia progression on one eye - something that my ophthalmologist retinal specialist originally was going to conclude the same old “nothing you can do about it” - until I asked about the experimental approaches I was aware of from my computational biochemistry background - including gene therapy). A dangerous approach if one believes off-label or experimental approaches may be warranted when it comes to “uncurable diseases” but doesn’t “speak up” and have someone who cares enough to take a look because they assumed you got it from a “health guru” from Dr.Google if the expert hasn’t heard about it. As soon as I mentioned my research background and credentials, my ophthalmologist took me completely seriously to gather research contacts.
If they stopped their meds based on a single-dimensional approach of presumed death, these participants could have lost their shot at the day when we finally have a much longer healthy lifespan with more evidence at maybe an exponential level. Every year may count for an extra 2 years.
So while it is true most of the time in those terminal situations, in short - it depends. I personally don’t rely too much on overly simplistic heuristics without fully understanding the limitations and really drilling on all the possible limitations. Some people prefer to not look as it’s not a priority or a very low priority to them. I’ve met a few physicians who believe all anti-aging is either a scam or should not be pursued (reasons from Neo- Malthusianism overpopulation to religious).
But this is a very high priority to me. I respect other people’s beliefs in how they want to handle their health, but for my own situation it may be different.
Lol seems even our posts reflect our tendencies. Mine concise yet effective. Yours verbose and meandering off point… Don’t worry, I jest.
I do however think it’s basic science that you only test one variable at a time. I take creatine since 25 years of experience and supporting research show it improves athletic and cognitive performance. I take rapamycin as it’s the most promising molecule for longevity. Hopefully my case study lasts another 60 years but in the mean time I’m happy with the immediate health benefits…
TF: What supplements do you take other than intermittent Rapamycin?
MK: I don’t take supplements… though my wife tries to get me to take vitamin D
Amen brother
We’re basically case studies for our children and the next generation. If I’m still healthy and active at 90+ then I can say with reasonable certainty that Rapamycin has been effective. If I’m also taking a dozen other supplements then you simply can’t tease out individual benefits (or impediments). My ‘data’ would be near worthless.
Not keen to get into the weeds on this one. My diet is typical of my culture and is not too dissimilar to my parents and grand parents. Ergo, any difference in lifespan or healthspan must be due to other variables.
I have a different approach - a lot of supplements I take can be found in food within a range or I just eat food directly, but they affect gut bacteria and nutrition similarly to the ones that Okinawan centenarians already took for 100+ years.
The difference is I check every single one because of rapamycin and a minimal amount of prescriptions due to my condition. I added rapa after the full stack - everything one by one - with washout/crossover
" If I’m also taking a dozen other supplements then you simply can’t tease out individual benefits (or impediments). My ‘data’ would be near worthless."
I don’t care about your “data”.
So, you only take rapamycin to prove a point?
You or no one else knows if supplements plus rapamycin will or will not make you live longer.
I am betting rapamycin plus other supplements with a lot of studies behind them such as metformin will extend life longer than rapamycin alone.
I am not recommending that anyone else take additional supplements, that’s their choice.
Metformin didn’t even extend lifespan in the ITP so that holds no interest to me what-so-ever.
Acarbose and 17a Estradiol look promising but, as I’ve said elsewhere, I do not believe benefits will be additive. If you look at the raw data from the ITP the longest lived single mice are actually outlier female controls. These interventions are certainly pushing up the median and the 90th percentile… but there still seems to be a hard limit to the absolute maximum.
That’s true, but if we were to say just look at only published, this specific “ultra-minimialist” belief doesn’t hold water either when you look at rapa + met.
If one is still skeptical about combination drugs in multicenter - it should be quite easy to test biomarkers using alternate dosing regimens on yourself (which I am doing) and watching alternate dosing protocols on animals - this should produce plenty of evidence to show synergistic effects.
There are some downsides to living longer. Which may become a negative side effect of taking rapamycin that you will have to deal with in the future.
At 81 years of age, I am the last of my family generation.
My brother and three sisters have all died.
My wife, who truly was the love of my life, succumbed to breast cancer after 53 years of marriage.
Virtually all of my longtime friends and co-workers have died.
I have outlived several nephews.
Fortunately, I have three wonderful daughters, one who is living with me, several grandchildren, and one great-grandchild.
It is also sad, but a part of life, to lose so many of our wonderful pets along the way.
Next month I will be attending a lecture which most of my co-workers will attend if they are still alive. Hoping to see some familiar faces and old friends.
Very interesting, if you look at mouse chow, it’s disgusting. No wonder they live so much longer on CR…they avoid eating that crap!
But why is he singling out Acarbose vs other interventions, the chow is uniformly equal? What about SGLT2 inhibitors, also glucose lowering and shows lifespan extension?
Mouse chow has been pretty much standardized in wild type mice since forever.
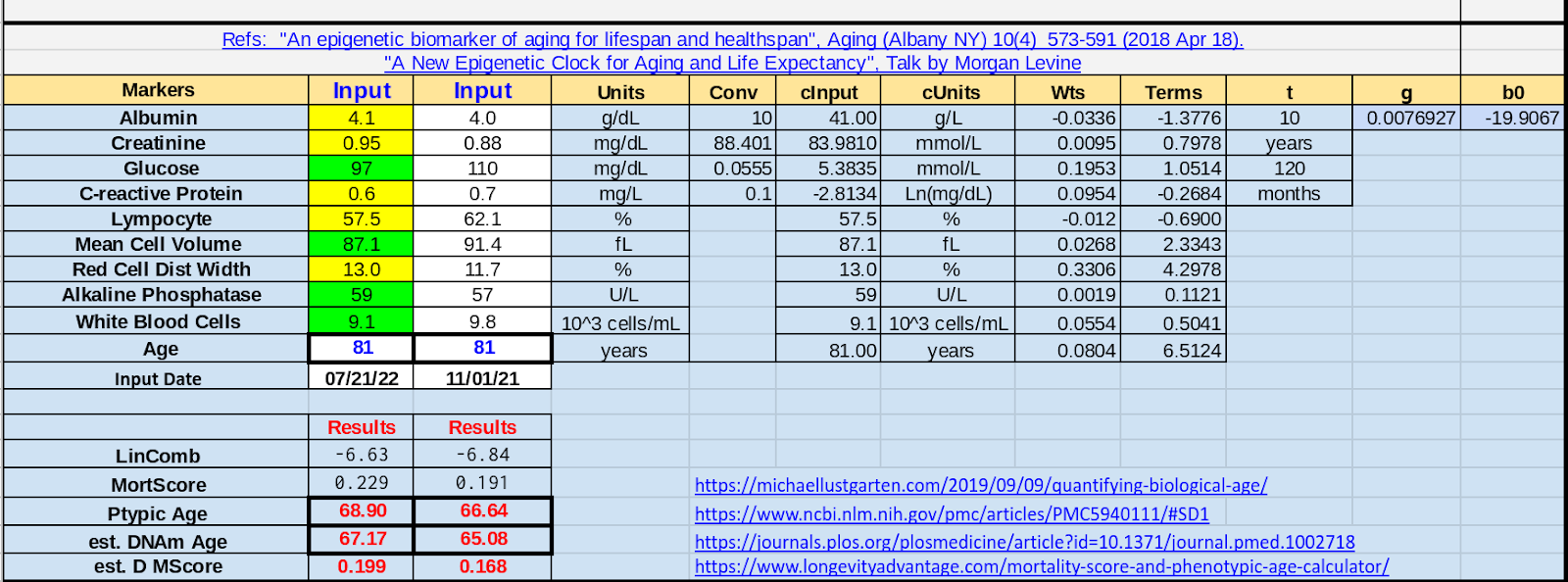
So, I plugged in my latest numbers into a phenotypic age calculator after taking rapamycin for 8+ months.
So far taking rapamycin seems to be making me age faster, though I have had many positive results that are not placebo, like the complete clearing of my actinic keratoses.
Any thoughts on this calculator? I have never been thoroughly convinced of the accuracy of the calculator because it totally leaves out lipids and some other health indicators.
It says I have aged 2.26 years in 9 months.
The green shadings are the markers that have improved. The yellow shadings are the markers that have worsened.