@desertshores Do you have similar for red cell distribution width, the heaviest weighted parameter in the Levine phenoage?
Yes, but I don’t have a similar chart to plot it on.
8/5/2021 RDW = 12.1%
5/26/2022 RDW = 12.8%
One thing that probably had a negative impact on my marker is the negative impact that 2 doses of the Pfizer covid vaccine had on many of my good markers. I did not include them, only the before and after taking rapamycin for ~7 months.
Your absolute RDW association with longevity, and would have a large impact (lowers) on your Levine phenoage.
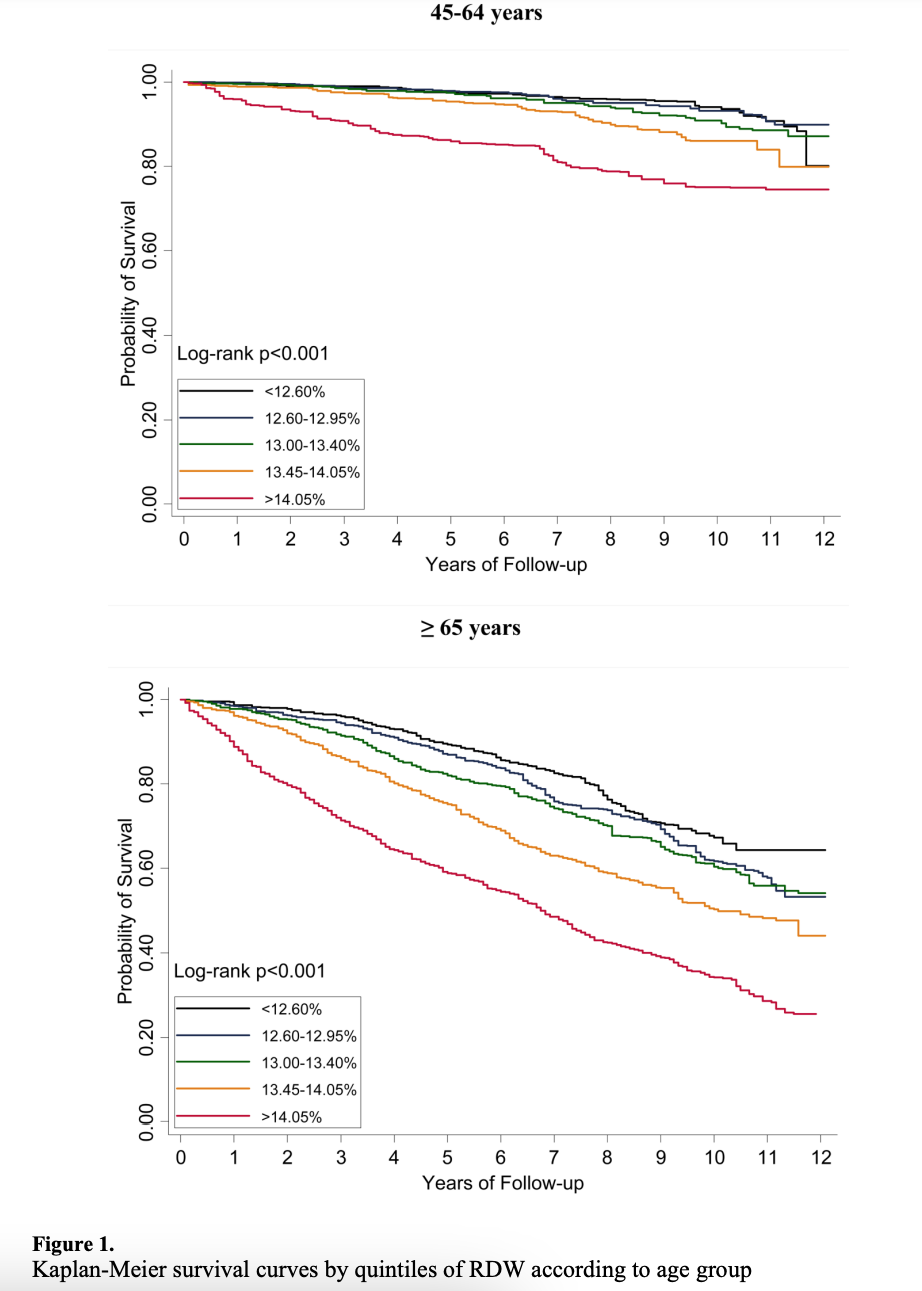
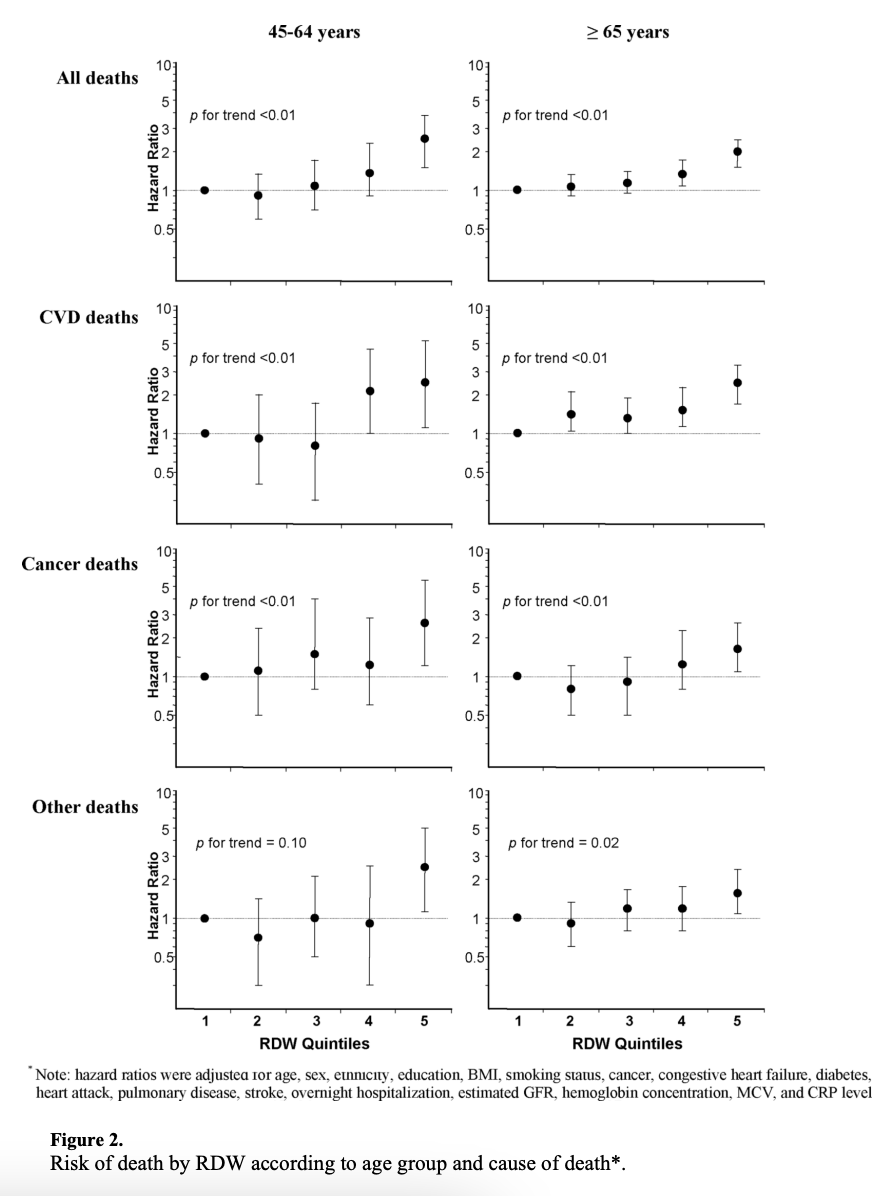
Red Cell Distribution Width and the Risk of Death in Middle-aged and Older Adults
Conclusions—RDW is a widely-available test that is a strong predictor of mortality in the general
population of adults aged 45 and older.
2 Likes
I had gotten a flu shot in Nov of 2022. There has been a discomfort in the upper arm since then and I never had any discomfort in the past from flu shots.
In researching I read where if a shot is too high on the arm it can cause pain but generally goes away in few months. It was down to a mild ache before starting Rapa. After I upped my dose to 6 mg with GFJ the pain has increased and certain movements of the shoulder really hurts. Even stranger is if I press on the arm, it does not hurt but making the certain movements sends a jolt of pain down the upper part of the arm. Going to continue the 6 mg for two more weeks then suspend the rapa for 30 days.
Sounds like you might be getting a frozen shoulder - just a coincidence that it has started developing at the same time as the flu shot. I doubt Rapa will help. You will probably need physiotherapy.
I had this years ago. There was one exercise that did the trick and that was from a standing position arms by my side, keep them straight and slowly raise up out to the side and keep going until pointing straight upwards. 10 reps twice a day - this was the one exercise from my physio sessions that made the difference.
1 Like
Thanks for the tip. I will give it a try.
I’ve had shoulder issues also in the past and physiotherapy (even relatively simple exercises that didn’t “seem” like they would do anything - were extremely helpful.
But, there is also evidence that rapamycin would help in this too. Matt Kaeberlein has said in the past that he thought rapamycin cured his frozen shoulder. It had been bothering him for many, many months - but when he started rapamycin it went away within a few weeks and has not come back. N = 1, so take it for what its worth.
3 Likes
Will note I’ve had easy bruising (only one bruise) at 8 mg, going to revert to 6 mg. I don’t recall any trauma to the area or anything. ~ 1 inch wide and no trauma. Other factors could be intake of ginger, turmeric, garlic, EPA/DHA and glucosamine (not supplements, from diet). No NSAID use. Pretty high Vitamin Bs, C, E and K1/K2 intake from diet. 1000 IU Vitamin D. 10g collagen peptides in bone broth per day. No bleeding disorders from WGS. Could also be Focalin XR but appears to be rare.

1 Like
Did the infections burn/itch? I never had herpes labialis before but just got them the first time this week
see Got my first ever herpes labialis / canker sore - #7 by RapAdmin
Just started taking Rapa - 1mg with GFJ - and of course, I got a canker sore. I was planning to keep slowly increasing my dosage until I got a side effect, and sure enough at 1 mg, there are side effects.
Should I back off the GFJ? Keep this level? Or keep increasing until I get something more severe? Thanks for the input.
2 Likes
I started at 1mg, and slowly increased by 1mg (no GFJ) and all worked well. I did get a canker sore once at around 6mg/week - but it went away, and never happened again. And I’ve continued upwards, and have tested as high as 25mg in a single dose (10mg + GFJ), no issues.
So, given my n of 1 experience, I recommend slower ramp than faster ramp. Starting with GFJ right off at the start seems a little aggressive by my experience… but again, n of 1, so take it for what its worth.
4 Likes
Thank you. ![]() I will take the advice to heart. The problem is these pills are too darn expensive!
I will take the advice to heart. The problem is these pills are too darn expensive!
Ah - thats why I like the India options: Buy Rapamycin Online - List of Reliable Pharmacies
At $1/mg for India-sourced rapamycin the cost for my coffee is probably higher per month than my rapamycin cost.
4 Likes
I’m waiting for my Indian courier to arrive in Hong Kong. They should arrive in 2-4 weeks. Until then, I am using Rapammune from Pfizer at $10 USD/1 mg.
2 Likes
And the drama continues. The courier said the package never arrived. The pharmacy shipped it to the courier. The shipping company said it was delivered to the courier. The courier is trustworthy so it appears someone intercepted the Rapamycin from the shipping company on behalf of the courier. The courier is investigating. This is starting to sound like a B grade movie… ![]()
This is what we do to get cheap generic Rapamycin.
Can’t you get Rapamune again? A 1mg rapamune tablet is almost as expensive as a 2 mg tablet, at least here in the Netherlands
I think this illustrates why being a minimalist or, better still, an essentialist is preferable.
1 Like
I like the way you think, but in Hong Kong they can only sell 1 mg or 0.5 mg tablets of Rappamune.
Good news. The courier received the shipment.
2 Likes
Well, I will note my regime is as minimal as it gets (I don’t take a bunch of herbal extracts and I don’t do stuff like GFJ etc and I time things to the point where unwanted drug-drug interactions theoretically are near zero - the rest are mostly monitoring if minor interactions but necessary. I don’t make a shotgun-style approach to gamble on a bunch of potential compounds that don’t have enough evidence) when it comes to getting 2 psychiatric disorders under control (ADHD literally screws me over on 12 healthy years if uncontrolled, and things like omega 3s are clinically significant if you ask any of the best research/professor type psychiatrists) - and trying to follow as close to what those Okinawan centenarians are doing with plausible mechanistic understanding for every single item. If anything comes up while careful monitoring, one can easily switch if they fully understand what’s going on when it comes to relatively minor reversible situations. (Which btw mild thrombocytopenia was reversed - I also am not on rapa temporarily for oral surgery prep)
I will also note that just wait till you need surgery or ICU (not hoping you do) - it gets extraordinarily complex when it comes to say wound healing or nerve stuff - an overly minimalist approach to nutrition (see what your surgeon recs on pre/peri/post op nutrition + immunonutrition - or lack thereof vs PhD/RDs in the best who are most up to date on the research and can prove it) results in much worse outcomes when compared. Not only that, wait till you see the overly “minimal” multivitamin recs some will make without any complex clinical reasoning (note many surgeons and physicians are not familiar with very in depth nutrition, so they just make overly simplistic recs that can be problematic. There are also a lot of charlatans in the nutrition field and way too much misinformation/ideology such that you have to really drill down the research and publication bias directly if you are a pragmatist - which I assure you very physicians have time for - it’s very low on priority but it’s my health) with plenty of perils of overly high amounts of certain vitamins/minerals or not accounting for complex supply chain/manufacturing issues. Two simple illustrations are supplement form alpha-tocopherol vs dietary gamma-tocopherols or supplemental beta-carotene from multivitamins in smokers causing higher mortality in lung cancer. Both in multis - even if the doc/pharmacist thought of going for a USP grade multi to cover manufacturing issues in a very simplistic way.
I always try to aim for “appropriate polypharmacy” when it comes to older adults who have to be on a very complex med schedule - just a huge number of tradeoffs. “Inappropriate deprescribing” is just as perilous.
Overprescribing and “inappropriate polypharmacy” is just as big a problem as underprescribing. Unfortunately, if an older adult is on enough meds because they have to, I often find they can’t easily find a geriatrician available.
2 Likes
My GF who’se an oncologist when she sees her patients she tells them they can quit their blood pressure medication (unless malignant hypertension of course)
and cholesterol lowering drugs because there’s no point in taking medication meant to slightly reduce the risk of dying from cardiovascular disease in a distant future when they are dead in a few months to years anyway. The same of course would also apply to the elderly, there is no point in prescribing preventive medication when you don’t have life expectancy left. Just enjoy the little time you have left without worrying about taking pills or the side effects that come with them
2 Likes