I’d like to discuss the pros/cons of SGLT2i’s and also compare them. I’ve only just started to do research on the topic. I found this 2022 review to be a great introduction.
The all-cause mortality data seems to favor Empa. " In the CANVAS program, compared with placebo, canagliflozin displayed a greater benefit on all-cause mortality in patients with a history of HF (HR = 0.70) than in patients without HF history (HR = 0.93) [72]. In EMPA-REG OUTCOME, empagliflozin reduced the risk of all-cause mortality by 32% (P < 0.001) [69]. In contrast, dapagliflozin did not notably lower the risk of all-cause mortality compared with placebo in DECLARE–TIMI 58 (HR = 0.93) [13]. In DAPA-HF, dapagliflozin reduced cardiovascular mortality to some extent (HR = 0.83) in subjects with HFrEF regardless of a previous history of diabetes [79]. There was a similar all-cause mortality between ertugliflozin and placebo (HR = 0.93) [11]."
Some other dimensions worth considering:
Safety / adverse events
Side effects
Interactions with other drugs/supplements
How well/long has it been studied and how many people have taking it
Thanks, I take Empagliflozin 25 mg, but started out on Canagliflozin 300 mg. Canagliflozin is more expensive for those that have to pay. Have got good results on losing weight and dropping glucose levels.
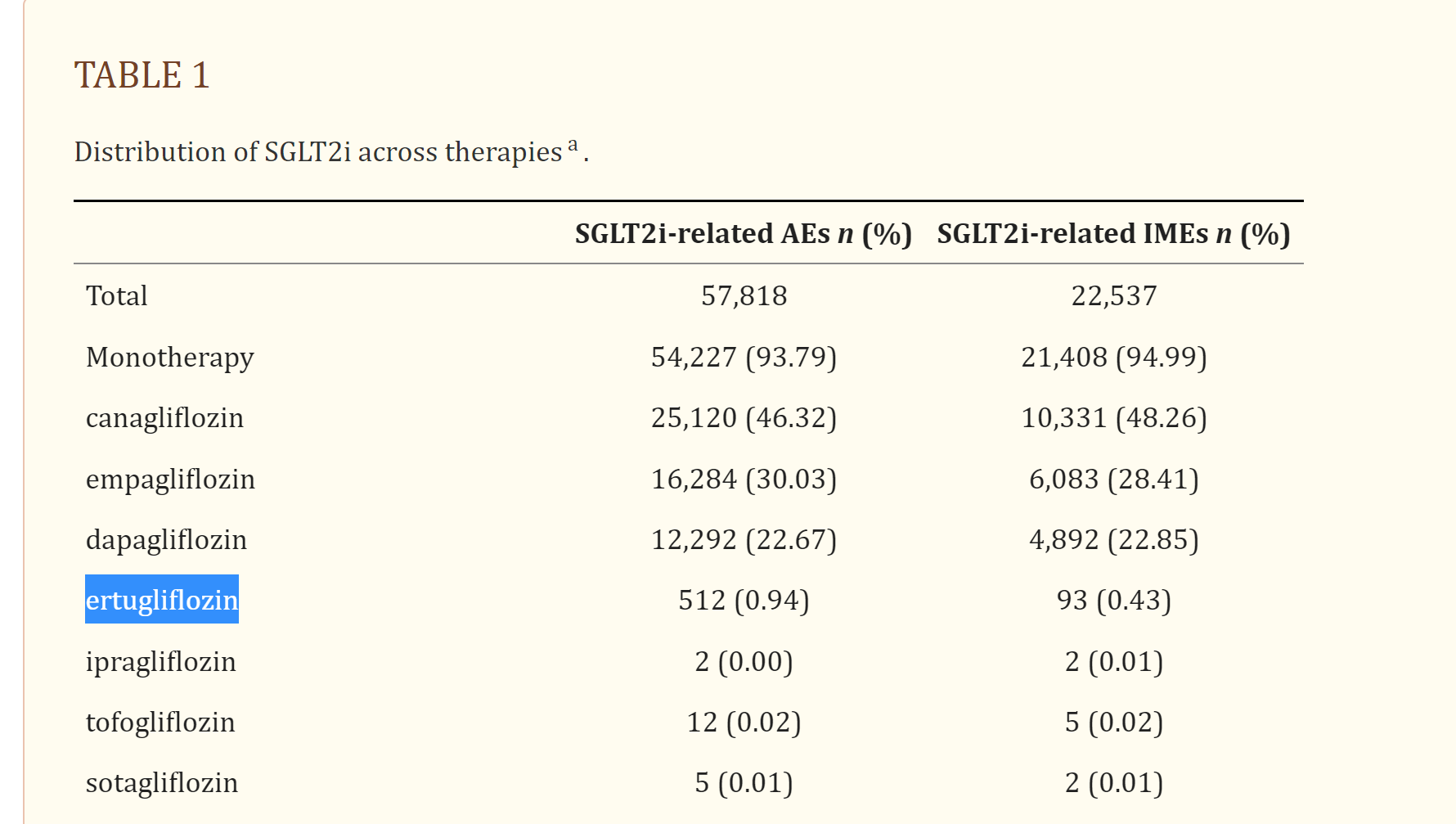
Caveat: I didn’t read this study, so not quite sure of context here. Maybe someone who has more time/expertise can take a look? Cause on the face of it, it looks like the very obscure ones have MUCH lower % AEs and IMEs than the more mainstream ones (i.e. I’m interpreting the “()” as a % cause that’s what is says at the top).
Ertu < Dapa < Empa < Cana ?
Ok I decided to look at bit at the paper. Does seem that dapa or ertu win on safety / AEs based on this.
Overall adverse events and adverse event-related discontinuation rates were generally similar between placebo, sitagliptin, glimepiride, and SGLT-2 inhibitors [99, 100]. However, canagliflozin 100 mg had a higher incidence of adverse events than placebo or sitagliptin [100]. The safety profile of empagliflozin was similar to sitagliptin or metformin, and most adverse events were mild or moderate in intensity [110]. Adverse events were similar between dapagliflozin and placebo, with few adverse events associated with volume depletion (< 1% vs. 0%) or renal function (1% vs < 1%) [89]. The most common adverse events related to dapagliflozin in DURATION-8 were diarrhea, injection site nodules, nausea, and urinary tract infection [121]. In DAPA-HF, the incidence of adverse reactions associated with volume depletion, renal insufficiency, as well as hypoglycemia did not differ between placebo and dapagliflozin [79]. The incidence of hypovolemia, symptomatic hypoglycemia, and urinary tract infection did not differ obviously between groups in patients receiving ertugliflozin compared with placebo or metformin [124, 125].
So considering safety (i.e. AEs) and efficacy (i.e. all-cause mortality reduction), seems that dapa is in the lead if you want safety and also require some stat sig for all-cause mortality reduction (which rules out ertu). Empa is in the lead if you want to maximize efficacy and are willing to take a bit of risk on AEs. Cana seems Paretto dominated by empa, in the these 2 dimensions as per this data set.
I would take all of this with a grain of salt. These are relatively new drugs. Most of the studies are comparisons to placebo, not to each other. Most of the studies are in diabetics not healthy people. Time will tell which is safest and which is best for long term health. As for weight loss, these are not considered to be the best class of drug for that.
I was thinking just as KarLT said; these drugs are for seriously out of control diabetics.
My wife is on the Levels CGM (continuous glucose monitor), or you may look at the cheaper https://to.nutrisense.io (cheaper CGM) AND being the dinner table observer of all her data collection and diet modification based on near real time glucose monitoring, and 2x to 5x a day ketone and uric acid testing (Dr Perlmutter’s book; Dropping Acid) my comments are:
Diet can 100% control glucose. IE if you only eat meat and near zero carb veges or like us no veges, just “carnivor” your glucose can flat line at 80’ish. No SGLT2 toxic junk needed.
Between rapamycin symulating caloric restriction benefits, and a bit of reasonable time ristricted eating, dropping to 2 meals a day; 11am and 4pm, you prob will gain all the possible benefits.
IMHO (just my opinion) these toxic drugs are of course developed for profit, but they would not be developed if Americans where the least bit compliant re modifying their diet.
The Paleo diet, now carnivor folks you can find on youtube claim 100% control of type 2 diabetes with just diet. I’ve observed my wife’s CGM data to be flat, 80’s, by only eating low/no carb foods. Her Uric acid (and mine) isn’t that bad (5’s). Perlmutters uric acid is 4.4, but he’s gone vegetarian and looks under nurished. But caloric restriction is a verified longevity strategy. (LOL). We have not seen high uric acid from a high protein diet!! Just us.
Sure experiment withg SGLT2 inhibitors, but why not drop your carbs first?? IE honest carbs / day <30g.
Why not wear a CGM? To me, an observer of my wife/s manic quest for health and “data” a CGM is an amazing health feedback device. So is ketone testing and uric acid testing. All doable at home.
BTW we go to the MHS, metabolic health symposium conference in Spring each year. A ton of researchers on low/no carb benefits. No talk of even metformin since its agreed that diet (very low carb) is a safer and more effective strategy then a STD diet + toxic drugs.
Best to all. Curt
PS I’m not tossing these pebbles lightly, I live in a very thin pained glass house. A litteral bushel of pills 2x a day, so many I have to run them through a blender to get them all down. I’m not pill-o-phobic.
For me, the key rationale for SGLT2 inhibitors is that while I avoid all refined carbs - I eat a lot of vegetables, and things like tomatoes, carrots, etc. can cause significant glucose spikes, and as we saw in the ITP program tests with Canagliflozin and Acarbose - these glucose spikes seem to be a significant factor in aging, especially for males. So - I take these drugs to moderate the glucose spikes, and for that purpose they are vey effective.
Thanks RapAdmin. I’m just offering my opinions and personal biases here and above. And thanks for illuminating your use of SGLT2 inhibitors!!! I would have said metformin would have been a help. But, I stopped taking metformin.
Alternatively; l-carnosine has been said to reduce the glucose metabolism byproducts (glucogen ??). I take 750mg morning and night. Reading these URLs tersely it appears carnosine reduces glucose AND insulin as well. Its insulin that is the main negative!!
To combat glucose I take: ALA, alpha lipoic acid 600mg morning and night, cinnamon, niacinamid (500mg 2x), benfotamine 300mg 2x, and l-carnosine 750mg 2x. And eat a very low carb diet, around 30g /day.
Not suggesting you go carnivor, but I have oberved many benefits, but it is an interesting observation reading your reasoning for taking SGLT2’s; so I can eat high carb foods and not suffer the negative consequences…
I’m terrible at humor, I would have worded my observation more humorously if I had that gift. ;(
Thanks to all for posting your self experimentation ideas and results. This is a fantastic forum!!
Ha! True. I eat a healthy most plan-based diet, I want to keep my blood glucose level as flat as possible, and I don’t want to have to worry about some vegetables and fruits that trigger the blood glucose spikes that seem to cause accelerated aging.
I also have higher lipid levels - and so a keto diet that is very high in fats is a problem too.
Interesting video, imo, on SGLT2 inhibitors as they relate to treating heart failure with or without diminished ejection fraction.
First 1/2 of the video goes into why echocardiograms are a crude 2 dimensional evaluation of the heart. This Dr. is one of the rare Youtube doctors who isn’t selling anything- he’s just a cardiologist trying to provide info to the masses. A bonus is that he explains things very well.