I can’t remember if we’ve discussed this newer study on this forum, but the results are a bit surprising. Orforglipron is associated with the greatest increase in HR (even though it’s a pure GLP-1 agonist) and tirzepatide the least. And the difference between tirz and reta is an average of just 1 extra beat per min:
4 Likes
12mg/week Reta and my RHR went up 8 BPM, but after a couple months maintaining that dose only up 5-6 BPM from baseline. Tirz up to 13mg/week maybe had a 2-3 BMP increase.
4 Likes
According to the trials, the average RHR bump with Tirzepatide is 1-4bpm and Retatrutide is 4-10BPM. But anecdotally, we see people online reporting very high RHR bumps with Reta. It makes sense that an obese person who loses tons of weight would drop a few bpm but the drug raises it. For people who aren’t obese taking them, the increase could be more since they aren’t dropping as much body fat.
3 Likes
This is a new article in The Atlantic, taken from behind curtain.
Is It Aging, or Is It ADHD?
by Yasmin Tayag
Realizing that your brain is slowing down can be jarring. After the age of, say, 45, anyone might start forgetting names, misplacing items, or struggling to pay attention, and the onset of such symptoms can often prompt a visit to a doctor, if only to confirm a patient’s hunch that the passage of time is to blame. Yet, as ever more of the United States’ aging population enters the “What’s happening to my brain?” stage of life, many patients are asking a new question, providers told me: Am I just getting old, or do I have ADHD?
In recent years, awareness of ADHD has spread dramatically—CDC estimates from 2020 to 2022 showed that roughly 11 percent of American children aged 5 to 17 had received a diagnosis. Now many Americans in midlife and beyond have started to question whether their cognitive chaos really is just a symptom of aging. For at least some people, the answer might very well be that they have undiagnosed ADHD and that the symptoms are becoming too prominent to cope with. Because the condition manifests differently as people age, the answer can also be “both.”
Historically, ADHD was closely associated with overactive boys. But global studies suggest that roughly 3 percent of people older than 50—which would translate to about 3.6 million Americans—are expected to have ADHD, David Goodman, an expert on adult ADHD at Johns Hopkins University, told me. Tensions persist around whether, in general, ADHD is overdiagnosed or underdiagnosed. But as awareness continues to rise among providers and the general public, diagnoses have been climbing in populations that were previously overlooked. The CDC reports that prescriptions for stimulants increased “substantially” among people in midlife from 2020 to 2021.
Midlife can complicate the already tricky process of diagnosing ADHD, though. Adult ADHD was directly addressed in the DSM-5, the American Psychiatric Association’s handbook of diagnoses, only in 2013, and it’s barely touched upon in medical schools, so many providers don’t think of it as a possible explanation for a patient’s worsening condition, Goodman said. As I have written previously, the only clinical guidelines for diagnosing or treating ADHD focus on childhood, and the disorder can show up very differently across the lifespan. For example, what looks like physical hyperactivity in childhood may manifest as internal restlessness later in life. Few physicians are trained to treat adult ADHD, and even those who are might struggle to tease apart the disorder’s symptoms from those of other health conditions that arise in midlife.
Read: Adult ADHD is the Wild West of psychology
The potential causes of declining cognition in midlife are numerous and frequently intersect. The shifts associated with “normal” aging can partly be attributed to the natural shrinkage of the brain and a decrease in the number of its neuronal connections. Mental- and cognitive-health consequences similar to those of ADHD can arise from psychiatric conditions that are prevalent in midlife, such as depression and anxiety. Mild neurocognitive disorder, a stage between healthy cognition and dementia that is common in people aged 65 and older, also has similar signs as ADHD, including missing appointments and frequently losing things. (Crucially, people with MND, but not ADHD, tend to forget words and how to spell them.) For some people, early-onset dementia or Alzheimer’s disease may be behind the symptoms. Caregiving, physical ailments, and increased work responsibility—all hallmarks of midlife—can exacerbate cognitive issues caused by any of these factors. “It can be tricky to rule all those things out,” Dara Babinski, a clinical psychologist at Penn State who studies ADHD across the female lifespan, told me.
Middle-aged women are particularly difficult to diagnose with ADHD. That’s partly because girls are less frequently diagnosed with ADHD than boys are, so many adult women live their whole life with the disorder without ever suspecting it. It’s also because many middle-aged women are dealing with perimenopause, which comes with cognitive changes such as brain fog, trouble concentrating, and forgetfulness. The fluctuations in hormone levels that cause perimenopausal symptoms can also exacerbate ADHD by interfering with dopamine signaling in the brain, Brandy Callahan, a neuropsychologist at the University of Calgary who studies ADHD in older adults, told me.
Increased awareness of adult ADHD, thanks in part to social media, has led many women to seek help for their symptoms, Babinski said. And stimulant prescriptions have risen especially sharply among women aged 50 to 54. Still, the combination of hazy diagnostic criteria and overlapping symptoms means that many older Americans with ADHD very likely don’t have a diagnosis. Even fewer are being treated, and so people may be having a worse experience of aging than they need to. A first-time diagnosis in midlife can profoundly improve the experience of aging. For one thing, it makes people feel validated at a time when major life changes can make it harder to cope with the effects of ADHD, which can include trouble maintaining relationships, paying bills on time, and performing at work. And a stimulant prescription can lead to improvements in attention, impulse control, and hyperactivity among people with ADHD.
Read: ADHD’s sobering life-expectancy numbers
Aside from improving life in middle age, a diagnosis has implications for future brain health. ADHD is associated with neurodegenerative disorders such as Alzheimer’s disease, Parkinson’s disease, and some types of dementia, but scientists aren’t yet sure why. One possibility is that people with ADHD struggle with habits that maintain a healthy brain, such as managing stress and getting adequate sleep and exercise, Craig Surman, a neuropsychiatrist and a scientific coordinator of the Adult ADHD Research Program at Massachusetts General Hospital, told me. Callahan and others have shown that ADHD brains have abnormal white matter—the communication pathway of the brain—which may make them less resilient to later disease. Researchers don’t know whether ADHD drugs actually protect against the underlying causes of more debilitating brain diseases. But if stimulants enable a person to maintain other habits that protect brain health, it’s reasonable to suspect that they might help.
Yet stimulants aren’t prescribed to older adults as often as they are to younger people. Most ADHD drugs are FDA-approved only for people up to age 55 or 65 because they haven’t been tested in anyone older and, as such, aren’t typically covered by Medicare. Stimulants also raise blood pressure and heart rate, which can be especially risky in midlife and later, when health issues such as cardiovascular disease and obesity are common. For these reasons, some providers are hesitant to prescribe stimulants to older adults. (The federal government, too, in the Make America Healthy Again report, argued that the drugs are overused.) But evidence is growing that prescribing ADHD medications to older adults can be done safely. This makes a reliable diagnosis all the more important.
The American Professional Society of ADHD and Related Disorders, known as APSARD, is expected to release the first clinical guidelines for adult ADHD this year. It’s an attempt to “put out some ground truth about how to treat ADHD,” Surman, who is on the guideline committee, told me. (He would not say whether APSARD will include specific guidelines for middle-aged and older adults.) Still, information is slow to disseminate, and there is pushback against the notion of adult ADHD from within and outside the medical field. Some providers feel that the risks of treating older adults with stimulants are not worth the benefit; other providers are concerned that the diagnosis over-medicalizes normal aging.
Yet as the American population skews older, perhaps it is worthwhile to question what constitutes normal aging. The medical literature offers only a loose definition: Rapidly deteriorating cognition is not normal, but gradual decline with age is. At the very least, the rise in adult-ADHD diagnoses presents an opportunity to refine the latter notion. No one’s brain stays sharp forever, but some people may have more time to maintain their edge.
2 Likes
Thank for sharing this @Tim, very interesting.
I had my brain scanned at Simon One last year, so I’ll have to look up the results again to see what it shows about my white matter… because, as per usual, I forgot ![]()
I never suspected I had it growing up because, as he article pointed out, I thought it was more about being hyperactive or having behavioral issues. Mine manifested in not filling out expense reports or paying bills on time… anything admin related.
I only learned a few years ago that memory problems were also part of ADD, so I was comforted to know why I had that lifelong issue. The nice thing is my memory has not become worse with age, but some other people are starting to catch up so the playing field is starting to level out.
I have endless memory stories, but the earliest one is they assigned me to be the hare in The Tortoise and the Tare (I didn’t ask for it but it was probably because I was outgoing at a young age), and they quickly turned me into a tree or something like when I couldn’t remember my lines ![]()
Not thrilled to see ADD brains might be more inclined to get neurodegenerative diseases… on top of everything else I have!
2 Likes
I found this interesting… from a new fiber-focused research paper:
The researchers also found that those with an above-average fibre intake had a slightly lower heart rate during the night than those who consumed less. A low nocturnal heart rate suggests that a person has entered a state of deep rest and repair, which puts less strain on the heart. “A 1 beat-per-minute difference [as observed between the high- and low-fibre groups] might not be that important for one night, but if that difference is sustained over decades or a lifetime, that could make an important difference [for cardiovascular health],” says St-Onge.
See: Butyrate: The Microbiome's Anti-Aging "Kill Switch" for Senescent Cells - #139 by RapAdmin
4 Likes
Link to study?
1 Like
Here’s the study the tweet was referencing. https://onlinelibrary.wiley.com/share/5BZXUGEAN6E7W3GFCUZB?target=10.1002/oby.70137
3 Likes
That’s pretty funny, you can buy those pens all day long on Alibaba as well as the empty cartridges.
1 Like
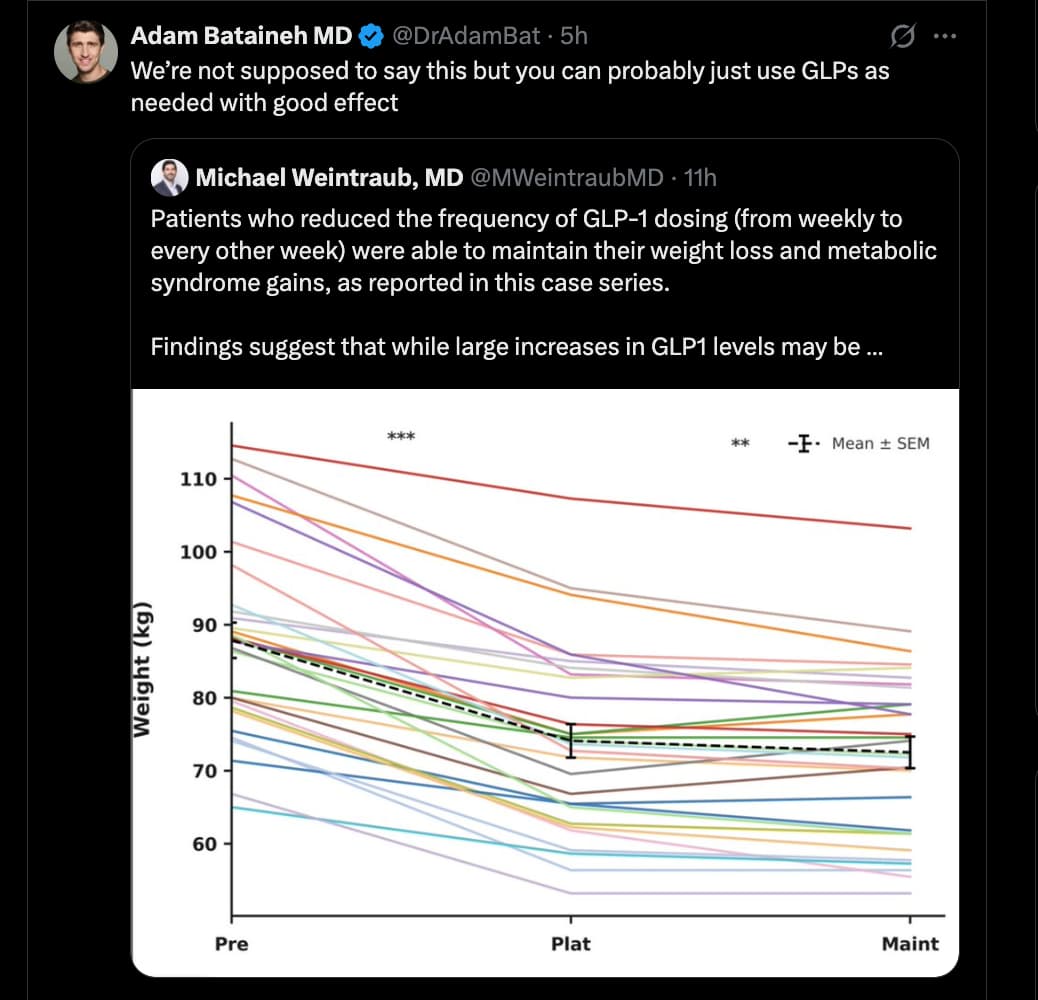
Most Patients Keep Weight Off With Fewer GLP-1 Shots, Study Finds
The doctor kept hearing the same story from his patients. After taking GLP-1 weight-loss drugs and finally shedding those excess pounds, some had gone a bit rogue. They began spacing out the shots instead of injecting themselves every week.
And it seemed to be working, said Dr. Mitch Biermann, an obesity and internal medicine specialist at Scripps Clinic in San Diego.
“By the time the third person told me they were taking it every second or third week and still maintaining their weight, I started recommending it to other patients,” he said.
Dr. Biermann also conceived a study to test the strategy. Now the results of that research are in: After 36 weeks of follow-up, most of the patients who spaced out their GLP-1 injections kept the weight off and also maintained health benefits like reduced blood pressure and better blood sugar control.
Only four patients gained weight after making the switch, and they quickly reverted back to weekly injections, the report said.
The study was small, only 34 patients in a relatively homogeneous group — mostly white and privately uninsured. And it was done by analyzing their existing medical charts.
Still, the research, published in February in the journal Obesity, provides a potentially appealing new option for patients who are loath to commit to lifelong weekly injections of a costly medication that may not be covered by insurance and that some fear could have unknown side effects.
Full article: Most Patients Keep Weight Off With Fewer GLP-1 Shots, Study Finds (NYT)
4 Likes
Probably because you are eating less.
1 Like

This doesn’t make any sense. If he drew up the medication successfully from the vial, there’s no reason to put the needle cap back on. Even if he did put the needle cap back on and forgot to take it off, he wouldn’t be able to even push down on the plunger if the needle cap is on because it blocks outflow from the syringe.
2 Likes
Never underestimate the sheer incompetence of your average redditor.
5 Likes
Or maybe just some random Reddiot trying to get attention by making up a story about the placebo effect.
6 Likes
If he was using an injector pen, there are 2 caps, the outer large cap and a small inner cap.
I’ve had several people do this exact thing, One did it 2 consecutive weeks.
I’ve done it once when I was in a hurry but I noticed it right away and re-did the shot.
2 Likes
Not sure if anyone has seen this report on GLP1’s and inflammaging.
2 Likes
Same. I had extremely unpleasant, almost (not almost, but exactly) psychiatric episodes of grieving sorrow, using 4-5mg of terzipatide. Not just “emotionally flatness”, but strong chemical depression. Without bad thought of selfharm,or self-blaming, just a feeling of extrem sadness whithout any reason. I almost quit because of it. Lowered my dosage to 3mg, went on plateu. Now slowly titrating, on 6mg. But a bit scared if it will return.
What about reta? Any similar adverse effects?
2 Likes
I’m interested as well. I had to quit semaglutide due to intense depressive and suicidal thoughts.
1 Like