Does there happen to be any biochemist on board… ? I would be extremely grateful for some insight into the structural and functional implications of a cysteine-to-alanine substitution in a peptide (as described in a patent) that eliminates a disulfide bond. I’m particularly interested in how this modification might affect folding and stability, and whether it could significantly impact its biological activity.
That sounds like an alphafold type of question
1 Like
I don’t really consider myself a biochemist but alanine substitutions are generally a stratagy to put a relatively inert filler aa in the place of one that you think has significance in the peptide or protein’s activity/stability. Cysteine Cysteine disulfide bonds are a biological solution to hold a protein in its 3-D structure. So molecular biologists often perform alanine substitutions to knock out a stabilizing bond between two loops of a peptide or protein. This could be used as a blind mutagenesis strategy where every cysteine in a region was substituted for an alanine and then proteins were screened for properties of increased or decreased structural sensitivity by looking for temperature-sensitive (either cold or hot) mutations. These were valuable tools because the activity of a protein could be modulated by say growing yeast carrying the mutated proteins at a couple of degrees warmer or colder than usual and then controlling the experiment with growth where the protein was stable.
In the case of peptides these bonds might be critical for the peptide activity since peptides lack multiple long secondary structures (beta barrels and alpha helices) that also contribute to the folding and stability and I would think substituting a known peptide disulfide bond with an alanine would have a huge effect on the stability of a peptide, likely destabilizing it and making it inert.
If you were looking for the affect of an alanine substitution in a specific peptide sequence to predict a change in protein folding then I’d agree with John that computer modeling of protein/peptide structure would be the way to investigate it.
2 Likes
Why not opt for Ibutamoren? Grehlin receptor agonist, orally bioavailable, proven by FDA trials to raise endogenous HGH almost as much as the jab (noninferior). And one less thing to inject, with all the risks of that.
Wrong, Ibutamoren is not approved by the FDA, because of concerns of congestive heart failures, and excessive edema. Iparemorelin, another ghrelin agonist seems to have comparatively less side effects and is more selective regarding cortisol and prolactin elevation. Iparorelin is also not FDA approved.
4 Likes
I used Perplexity to put this together.
maybe 10 minutes of my input ![]()
Lots of interesting benefits with GLP1’s
GLP1RA_Inflammaging_Report.pdf (102.7 KB)
4 Likes
Did you end up trying this? I’m thinking of getting BPC157 capsules to see if it can improve gut health. Sometimes I get indigestion and stuff and know when this happens I feel some autoimmune conditions get a bit worse so there might be a connection there.
Who has tried it and does anyone know a good affordable source of BPC157 capsules?
2 Likes
Floxed - a serious untreatable condition brought on by an allergic reaction to the ciprofloxacin antibiotic (and it’s 'floxacin relatives) .
Cipro is a black label antibiotic due to the severity of an allergic reaction with this one. This means it’s an antibiotic of last resort. Incredibly useful in most cases. Problem is, you don’t know who is allergic until it happens. Then it’s too late.
Our daughter was “floxed” about 8 years a ago and has suffered extreme neuropathic pain from her calves to her toes, it varies in severity but has never gone away until now. She has other symptoms but this one was the most prevalent for her.
We tried a number of things over the years and nothing would touch it.
She was visiting us this weekend and commented that the neuropathic pain is now gone. She noticed that about 2 weeks ago. Funny how when things get better it can sneak up on us and quickly become the new “normal” It took her a few days to recognize this was not a transient improvement. That it seems to be “permanent” but time will tell.
What may have done this?
She has been taking a number of peptides over the years with no effect on this.
8 months ago she started on ARA 290 - 4mg per day, 5 days a week. Not an overnight change but she “thought” she was experiencing fewer high level incidents.
3 months ago we added SS 31 as being floxed does affect the mitochondria.
We are not sure which of these 2 or if it’s the combination has finally given her some relief but we are all pretty excited for her to finally be pain free after 8 years.
The severity of this condition for some is extreme, ruptured tendons, relentless pain, living in a wheel chair, etc. There are over 100,000 cases of this in the US so probably 10,000 in Canada, not to mention the rest of the world.
9 Likes
If she tried so many things without success I guess placebo can be ruled out.
1 Like
Since the vet forms of fluoroquinolone cause it in animals I think we can rule out it just being in the head. It’s very real.
1 Like
I think he meant the result in stopping the neuropathy ![]()
2 Likes
oops, I’m a little slow today.
1 Like
It’s About to Be Hot Peptide Summer (GQ magazine)
Brace yourself for hot peptide summer.
In late February, health secretary Robert F. Kennedy Jr. joined Joe Rogan on his podcast, revealing that that he’s directing the FDA to loosen regulations on over a dozen previously banned peptides. The move, which seems likely to be announced in the coming weeks, would largely reverse the FDA’s previous decision to place 19 peptides on the agency’s category 2 list, which effectively bans pharmacies from formulating them for human use—and, by extension, restricts doctors from prescribing them. (Not that the initial decision to ban these peptides prevented surging demand from fueling a booming black market online).
According to the Human Health and Services Secretary, who expects that about 14 of these peptides will soon be moved back to the right side of the law, the compounds should have never been banned in the first place. He cites overreach by the Biden administration, but the fact remains that virtually all of these peptides still lack meaningful—and in some cases, any—human trials.
That reality has many experts worried. For instance, in a recent paper published in the journal Current Reviews in Musculoskeletal Medicine, researchers at the University of Utah noted that the popular compound BPC-157, nicknamed the “Wolverine” peptide for its potential regenerative abilities, could theoretically also promote the growth of tumor cells.
All of that said, this isn’t necessarily bad news, considering the popularity of these peptides continues to surge, regardless of whether the FDA deems them naughty or nice. For one, moving a drug from category 2 to category 1, where it becomes fair game for pharmacies and physician-prescribed treatment, makes it considerably more likely to be researched more thoroughly. And for the increasing number of people seeking out these peptides regardless, allowing them to be processed in FDA-inspected facilities reduces the reliance on a murky black market fraught with its own risks.
Read the full article: It’s About to Be Hot Peptide Summer (GQ magazine)
1 Like
It seems that the grey market peptide world is getting squeezed…
source: https://x.com/pitdesi/status/2039823579731407221?s=20
2 Likes
I wouldn’t advise getting anything you inject or consume off Amazon anyway.
3 Likes
I won’t even buy syringes for my cats from amazon… but of course I put their safety over mine, so….
But it is an interesting developement!
1 Like
Good riddance, buying medical supplies on Amazon is not an adventure I would recommend having. Many bac water products on this site didn’t pass benzyl alcohol content and pH tests anyway. I hope this guy was buying Hospira.
1 Like
Interesting… I tend to go to Amazon for many things as they deliver next day. But it looks like Customs and the FDA are cracking down in a number of areas…
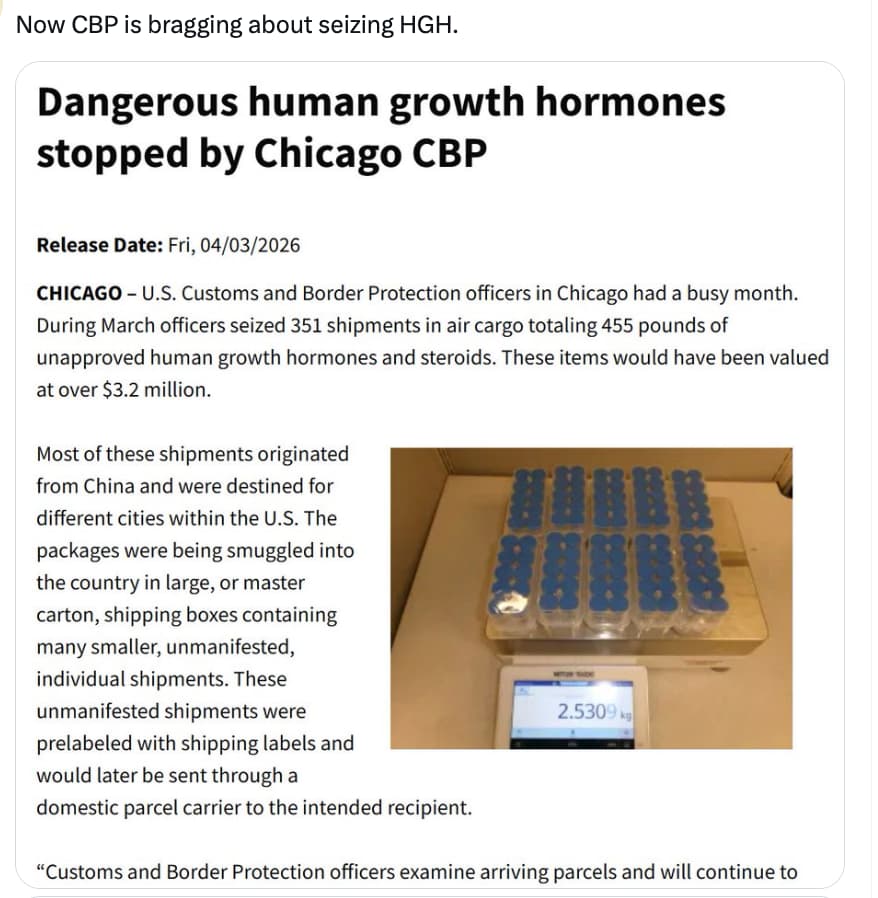
Source: https://x.com/cremieuxrecueil/status/2040542552642691476?s=20
Reading the tweet (and the quoted tweet) it looks like CBP are giving more attention to imports “smuggled”
Yes, many vendors have been affected by increased seizures lately. The war on Iran is not helping either. It’s a cat and mouse game, several vendors are in the process of changing routes.
I’m actually more worried about the impact of the war on manufacturing and shipping prices. We’re already seeing many Asian economies affected by oil shortages.