Not all statins have same CYP3A4 enzyme interaction, but several have a very strong AUC rise, so for sure, heed your doc’s advice or check the literature on your specific statin.
1 Like
Yeah, we have a lot to learn. But Matt’s 2014 summary of dosages and results helps a bit:
5 Likes
Do you have the link to this webinar? Thank you.
No - they have not distributed it yet.
I recommend you join the survey and they will send it to you when they have it available.
1 Like
It is agreed that prolonged mTORC1 inhibition eventually leads to mTORC2 inhibition. In humans, is it known how long this takes, or how long of a rapamycin washout period is required to replenish mTORC2 to its normal (pre-rapamycin exposure) levels? If not known in humans, is it possible to extrapolate a guess from the published mouse data?
I can’t find it now, but I remember Dr. Dudley Lamming (a well known mTOR researcher) had a series of posts on Twitter in which he showed (with multiple literature references) that mTORC2 inhibition provides no benefits from a longevity perspective, only detriment to lifespan.
Are there any references which detail whether the potential side effects of rapamycin (i.e. elevated glucose, dyslipidemia, anemia, lymphopenia) are mechanistically due to mTORC2 inhibition?
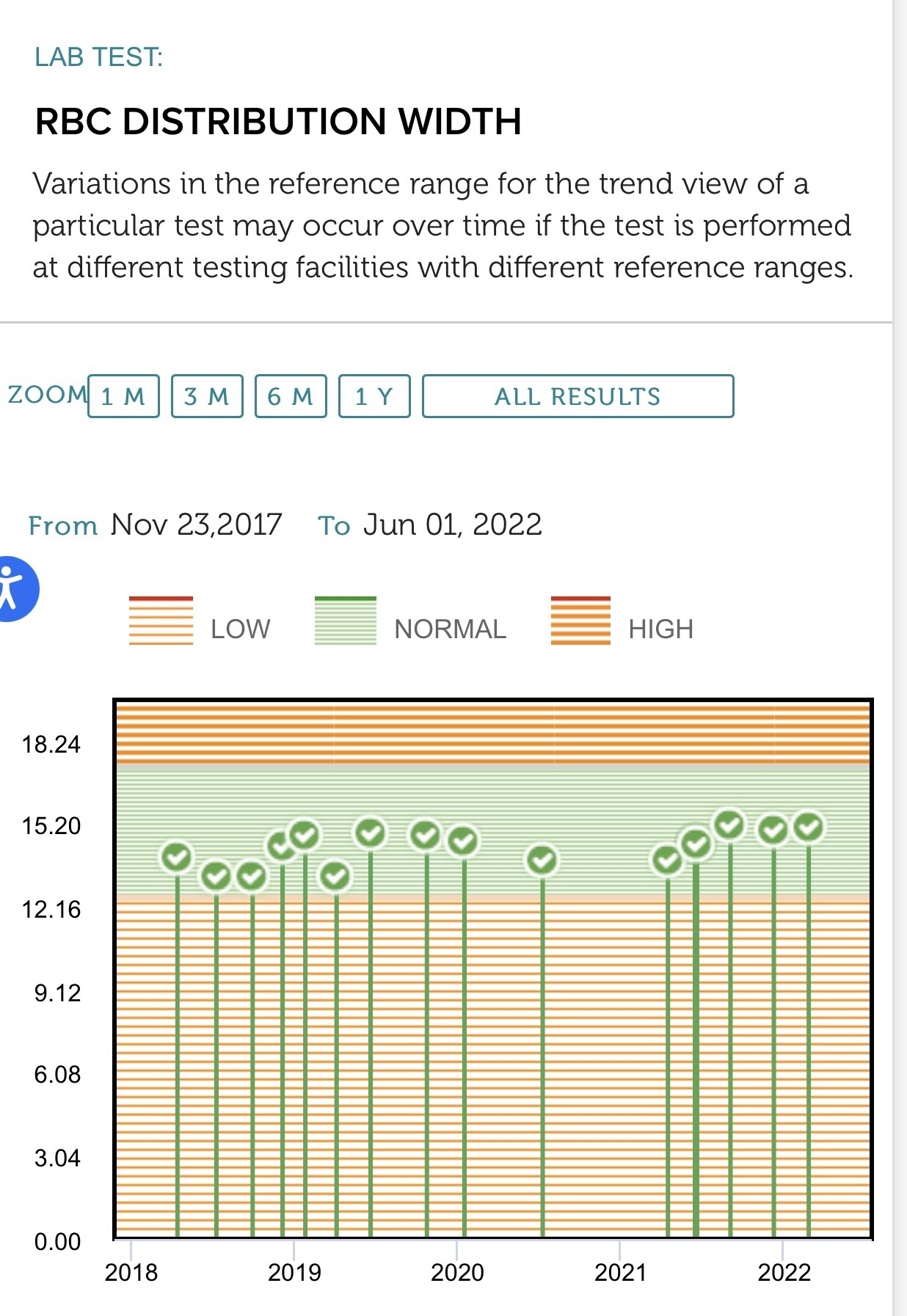
MAC, did you notice any increase in your red cell distribution width (RDW) since starting your blood donation regimen? According to the DNAm PhenoAge calculator, a higher RDW has the strongest correlation with higher phenotypic age. I noticed an increase in my RDW after donating blood.
1 Like
Yes - its know - see this post:
As far as washout - yes - thats just the blood/sirolimus level curve that you see here (extrapolate the curve out several more days to get to zero, depending on dose):
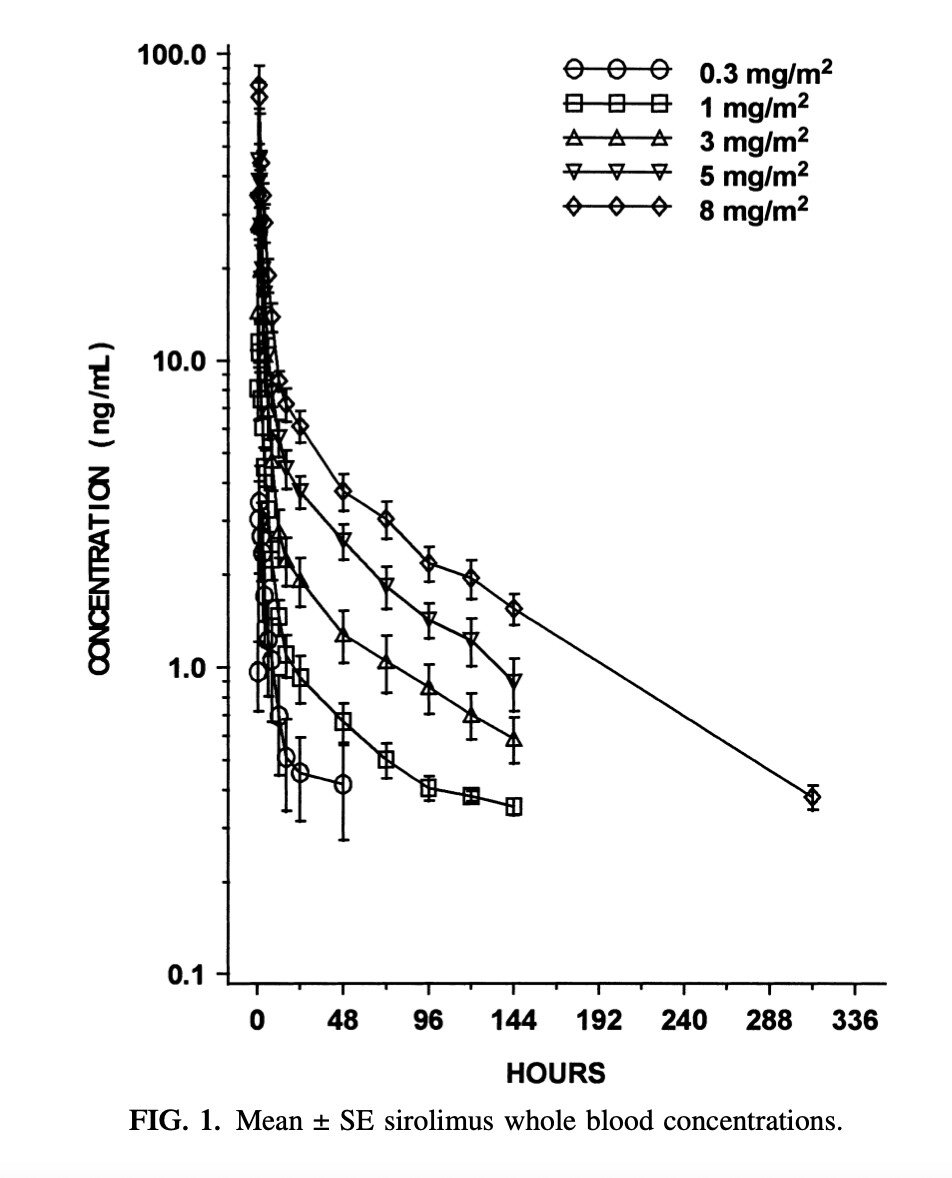
From What are the Typical Rapamycin Dosing / Dosage for Anti-Aging? - #8 by RapAdmin
Also, in the same interview, Lloyd Klickstein said, about the study with the rapalog everolimus:
- Each of the doses did a different thing to TORC1 inhibition…
- The .5 mg dose partially inhibited in a sustained fashion.
- The 5 mg once a week fully inhibited TORC1 for a couple days out of the week
- The 20 mgs would fully inhibit TORC1 over the dosing interval (i.e., nonstop inhibition of MTORC1 until your next dose)
Can we actually expect any additional effect from a dose higher than that necessary to “fully inhibit TORC1 over the dosing interval”? Do we have reasons to think that rapamycin (or a rapalog like everolimus here) acts (against aging) through other means than the inhibition of mTOR?
Green is taking 12 mg weekly. I see no reason you could not take 10 mg. weekly. Increase 1 mg weekly from where you are at until you get side effects, and then back off 1 mg. You are at the optimum dose for longevity purposes. I am 76 and take 20 mg. twice a month. Most people experiment with there own bodies to find best dose.
2 Likes
Thanks for your response. I am curious about the rationale for 20 mg twice a month instead of 10 mg once a week. Were you advised by a health care professional or just self experimenting like most of us?
BTW, on the AMA Dr. Green said he now takes 12 mg two days in a row (total 24 mg) and then takes 10 days off.
Exactly how did you arrive at this conclusion?
A few mouth sores or minor side effects equates to breaching a threshold and having escaped into longevity extension by Rapamycin?
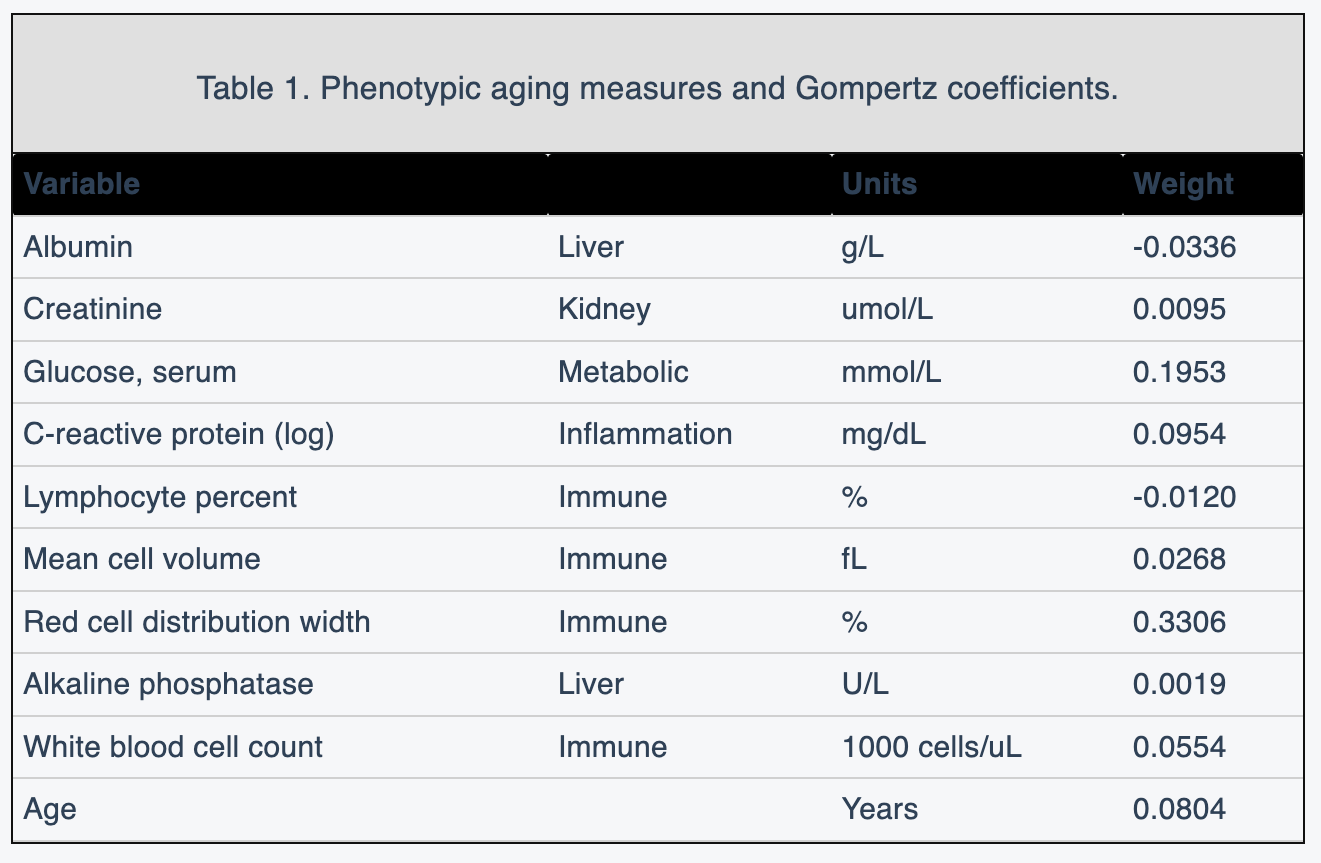
Re the DNAm PhenoAge calculator weighting, hadn’t realized RDW had such a high weighting, duly noted. Briefly parsing through the paper, it referenced a table on coefficients I could not find, can you give some insight mechanistically why it has such a high weighting?
1 Like
This is informative. So it seems to me that 5 mg/ week is a very good dose in that mTOR will be fully inhibited for several days, and then I assume will be partly inhibited for a day or two, followed by a couple of days of no inhibition. That sounds about right to me.
1 Like
I think that RDW is more an indicator of cellular size in general. Rapamycin decreases cellular growth and size and this should be reflected in the RDW. With blood donation you’re probably seeing younger replacement cells for a certain time period which would have a larger size . This wouldn’t be a reflection of increased cell size in general.
@MAC is that an app you are using to track our lab results? (from the image you posted it does look that way). can you share the app name. I’d like to be able to track my lab results over time like that…
Thanks.
Seems we know far less about mTOR2 than mTOR1, yet we seem to ascribe all the benefits of “Rapamycin longevity”, namely, the default chronically-daily-prolonged treatment-cancer mice model (unlike what us humans are doing), to mTOR1? But this is most definitely not true.
The Enigma of Rapamycin Dosage
“Rapamycin is a natural product that inhibits mTOR with high specificity. However, its efficacy varies by dose in several contexts. First, different doses of rapamycin are needed to suppress mTOR in different cell lines; second, different doses of rapamycin are needed to suppress the phosphorylation of different mTOR substrates; and third, there is a differential sensitivity of the two mTOR complexes mTORC1 and mTORC2 to rapamycin”
Targeted Inhibition of Rictor/mTORC2 in Cancer Treatment: A New Era after Rapamycin
“mTORC2 specifically senses growth factors and regulates cell proliferation, metabolism, actin rearrangement, and survival. Dysregulation of mTOR signaling often occurs in a variety of human malignant diseases, rendering it a crucial and validated target in cancer treatment. However, the effectiveness of rapamycin as single-agent therapy is suppressed, in part, by the numerous strong mTORC1-dependent negative feedback loops. Recent cancer biology studies indicated that mTORC2 is a promising target, since its activity is essential for the development of a number of cancers. These studies provide a rationale for developing inhibitors specifically targeting mTORC2, which do not perturb the mTORC1- dependent negative feedback loops and have a more acceptable therapeutic window. This review summarizes the present understanding of mTORC2 signaling and functions, especially tumorigenic functions, highlighting the current status and future perspectives for targeting mTORC2 in cancer treatment”
mTORC1 and mTORC2 in cancer and the tumor microenvironment
“While mTORC1 signaling has been extensively studied in cancer, recent discoveries indicate a subset of human cancers harboring amplifications in mTORC2-specific genes as the only actionable genomic alterations, suggesting a distinct role for mTORC2 in cancer as well mTORC2 in the center of cancer metabolic reprogramming”
“Here we review the recently identified central regulatory role for mTORC2, a downstream effector of many cancer-causing mutations, in metabolic reprogramming and cancer drug resistance.”
mTORC2 Promotes Tumorigenesis via Lipid Synthesis
https://www.cell.com/cancer-cell/pdfExtended/S1535-6108(17)30514-7
“mTORC2 promotes de novo fatty acid and lipid synthesis. This pathway is elevated in human liver cancer and drives hepatosteatosis and liver cancer in mice, whereas its inhibition or deletion of Rictor reduces mouse tumors, suggesting this pathway as a therapeutic target in liver cancer.”
3 Likes
@RapAdmin No, this is a portal into all my lab results, provided by the testing lab. I can filter by lab type and historical.
It’s certainly possible for dual mTOR suppression to lead to even greater cancer prevention. However, we also know that in transplant patients that they have a significant degree of immunosuppression supposedly from mTOR 2 inhibition. Not something that we would want.
What lab provides that? - very nice! All I get is a mailed PDF from my LEF/Labcorp results. Its a pain to manage or track over time.
1 Like