I just completed the Sirolimus blood test via LabCorp. My Rapamycin dose is 20 mg every two weeks and this test was done on the day before my next dose—so at the end of the dosing cycle. My results: <0.5 (low) and the range is 3.0 to 20.0.
Very Interesting! Thanks for posting. So this is called your “Trough” level of sirolimus. It is (roughly) the lowest point of sirolimus/blood concentration just before you take your next dose.
At the level you tested at (under .5 ng/ml) that suggests to me that you are being very safe, in terms of waiting / interval times between dosing. It would seem that the risk of the side effects seen with continual dosing (and therefore mTORC2 inhibition risk, as the current theory goes) seems low.
The challenge we all face is that we don’t know exactly what the trough level that is ideal for each individual person - and perhaps there is a tradeoff - higher dosing means better life extension, but higher dose and higher trough levels also increase the risk of side effects and potential immune system supression…
I hope some doctors or researchers weigh in here on their thinking about how people might use these trough sirolimus blood level tests to try to optimize the dosing, both individually and in the larger population of people who are taking this drug for anti-aging. I’ll add our doctor / researcher members to this post to let them be notified about it and I hope they’ll weigh in on this test results and how we can use them. @drsteve7777, @DrRoss , @DrT , @Drdml , @mTORdocTOR , @mkaeberlein , @lwd2000
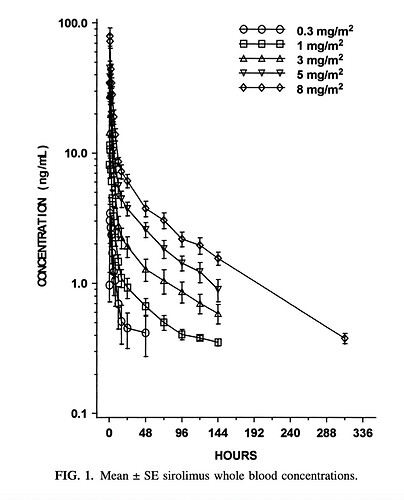
Here below is what the range of dosing curves that have been shown in healthy people dosed with sirolimus. These doses are in terms of surface area (m2) which is a little less common than what I’m used to which is mg/kg of weight. There is a calculator somewhere on the web that helps you covert the surface area calculation (mg/m2) to mg./kg. - and I don’t have it front of me. I seem to remember that the 8mg/m2 number translates into around 12mg dose for a 70kg person - but don’t quote me on that. Just for reference sake in terms of looking at this graph.
I just got my first LabCorp test for a trough (7 days after my weekly 3mg, which is preceded by GFJ three hours before and accompanying a fatty snack). My results were the same as yours: 0.5 ng/mL. Based on this, I plan to go up to 5mg/week with the same protocol, test for a peak (to make sure I have actual rapamycin), then re-test for a trough in a couple of months.
Based on the pharmakinetic data for Rapamycin, why not add a blood test (s) to try and catch a high signal, just to validate you (n=1) are getting a true Rapamycin dosing. You can also get a trough, and repeat as you iterate to try and max your mTOR signalling, whilst minimizing side effects.
The high signal is hard to catch I suspect. I’ve gone into LabCorp offices for my scheduled appointment and they are frequently 30 minutes to 80 minutes late in getting me into the seat for a blood draw. At least at my locale office - I don’t have much confidence that I could catch my peak sirolimus levels due to this uncertainty.
FWIW…if you have the resources consider doing the testing the same as in the study.
Multiple draws over the time, such as a base, take dose, 30 minutes, 1 hour, 2 hours, 3 hour, 4 hours, Yes at $95.00 per each draw test can add up. You will have real numbers for yourself.
Agreed. I have changed my Rapamycin supplier, and will doing such an experiment, drawing blood every 20-30 minutes for about 2 hrs. My lab cost is quite low where I am. Just plan ahead with lab, perhaps ask them when is a slower time, and explain clearly the protocol going in.
Important to keep in mind those timelines are for rapa absorption in the fasted stated. If you take your rapa with food to enhance overall absorption/AUC, it’s going to slow down absorption and delay the peak somewhat.
Good to know! Would be really helpful see Cmax and time variables for capsules vs tablets. I’d expect capsules to be absorbed much faster and possibly higher Cmax, unless the powder being released in the stomach interferes significantly with absorption.
Incidentally, IF it’s true that stomach acid interferes w/absorption of rapa (can’t remember where I saw this?), I wonder how much it might increase absorption to take an H2 blocker such as famotidine before one’s weekly dose?
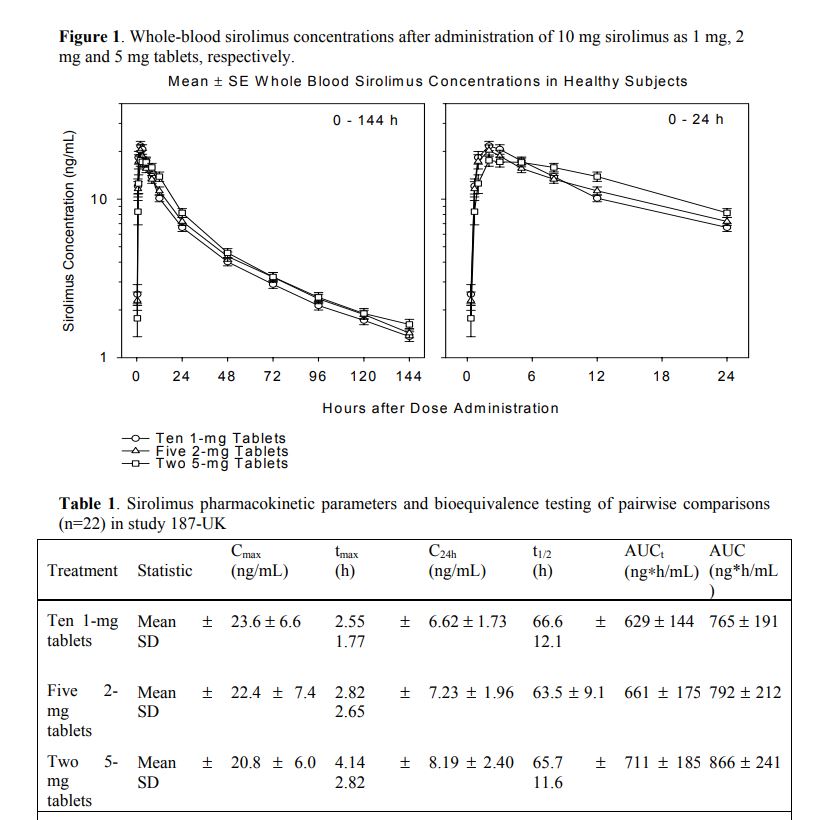
EnrQay, in the study you referenced, the study participants were given an oral solution containing 5 mg/mL sirolimus. In the other study I cited in this thread, the time-to-peak plasma concentration is significantly longer when taking sirolimus tablets.
Most studies show significant inter individual pharmakinetics within the cohort. So unless we’re doing well controlled dosing protocols AND in parallel blood Sirolimus testing, most of us are flying blind. From what I can survey from various forums, very few people are doing this clinical grade-like monitoring. Side effects might serve as crude upper dosing limit cutoff, but is it the Cmax and/or AUC that is responsible? And what about measuring other biomarkers that are associated with Sirolimus…kidney and liver function, lipids, glucose, CBC? Other proxy markers? I’ve started to do some of this testing, but plan to bring more detailed monitoring this coming year.
I got the results for my second sirolimus test from Labcorp (ordered through Life Extension). My previous result measured the trough (see my Mar 3 post above) at <0.5ng/ml 7days after 3mg rapa with earlier grapefruit and fatty snack at the same time as rapa.
This test was 1.75 hours after my weekly 5mg, which was taken with a fatty snack, and taken about 2.5 hours after eating 8 oz whole grapefruit. Some might interpret this as excessive rapamycin, since the GF might multiply the effect by 3 - 3.5x and the fatty snack might increase absorption by 1/3.
My results: 17ng/mL, which seems right in the therapeutic range. Have others here posted results? I plan to get tested again in a couple of months to test my trough at this higher 5mg dose.
Any comments? Too high? Not high enough? It seems in line, maybe on the low side, with the graph at the top of this page.
“For the sirolimus plus grapefruit juice study, sirolimus was administered alone in week 1 and with grapefruit juice starting in week 2, one day prior to sirolimus. Grapefruit juice (supplied by Florida Department of Citrus), 240 cc, was administered once daily without interruption. This dosing was based on research demonstrating that the half-life of intestinal enzyme inhibition of grapefruit juice is 12 hours(21) thus providing time for modulation prior to sirolimus dosing”
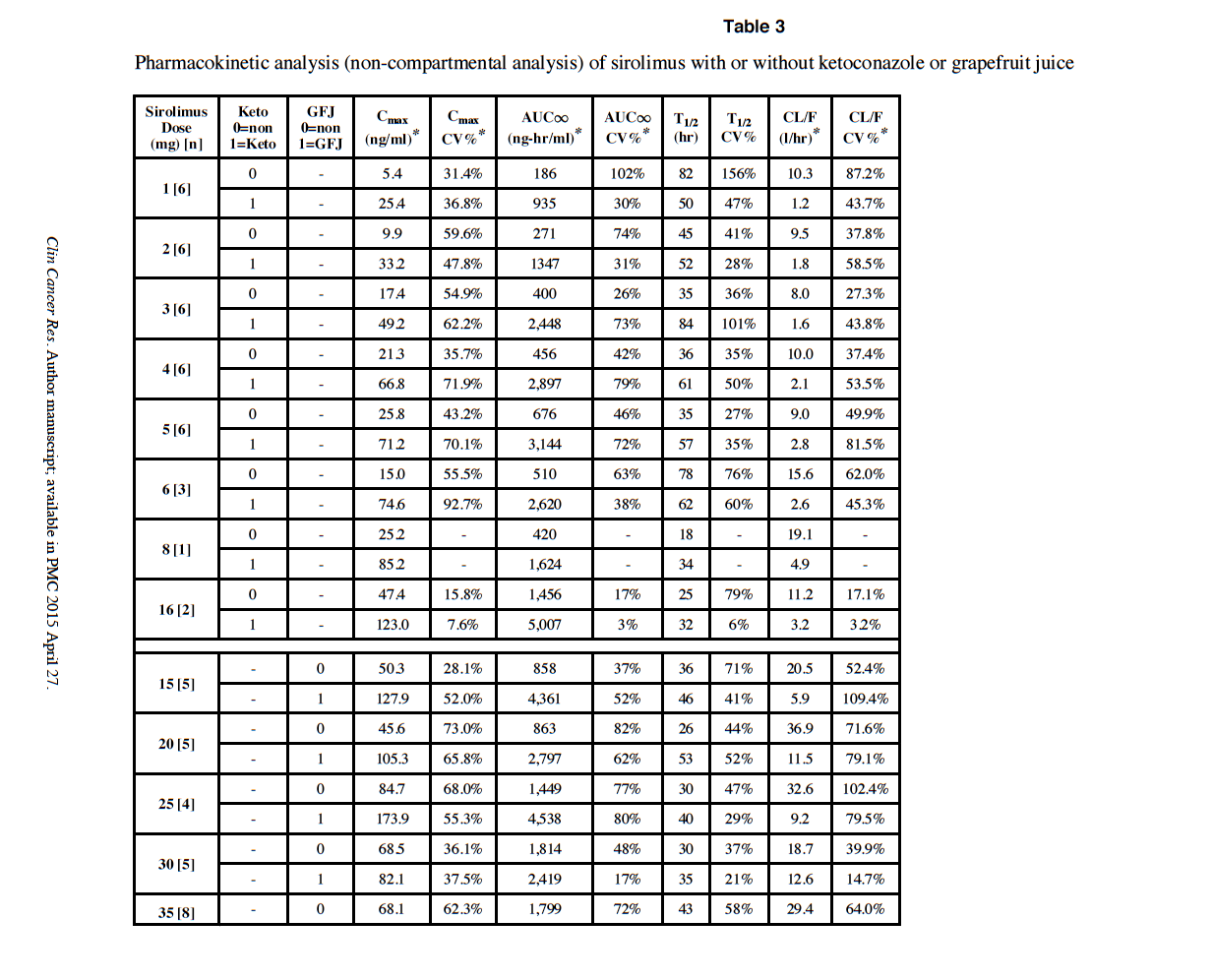
At 5mg with GFJ, Cmax in the study is around 70 ng/ml. As you can see, there are some Cmax over 100 ng/ml.
It’s the wild wild west for exploring the max without side effects. See Table 1 in the referenced study.
Yes, would be good to also get a trough measurement.
I am taking 12mg weekly with dual night before/morning of GFJ. But I’ve not fully vetted my Rapamycin current vendor.
I just got my new Rapamycin order, sending out for confirmation lab analysis, and then will redo a blood Sirolimus experiment, both trough, and trying to capture the signal after GFJ/dose. Will post.
If I am reading this chart right, 5mg rapa + ketoconazole produced Cmax=71.2. The grapefruit was tested only with 15mg-35mg levels. The 15mg +GF produced Cmax = 127.9. My own 5mg + GF produced Cmax=17. So, yes, if you scale down their 15mg to my 5mg, my Cmax seems low.
But the question remains, is this a good therapeutic range?
Yes - we really have very little idea here (at least in any specific, measurable way). Nor do we know how large the dose / response variation might be between people. Its frustrating to have so many unknowns around rapamycin.