No question - they are getting mTORC2 inhibition. I was talking with David Salmon who is running the marmoset rapamycin lifespan studies, and at 1mg/kg they are definitely seeing mTORC2 inhibition, but not much in the way of negative side effects (glucose or lipid disregulation), …
Obviously the benefits of mTORC1 inhibition outweigh the negatives of mTORC2 inhibition, in terms lifespan improvement (in animals living in pathogen-free environments).
@desertshores Thanks! I’ve learned a lot talking to those people. My perspective has shifted dramatically since I started doing the podcast. It’s a rich compensation.
No, my only point is that no one knows, not Dr. Greene, Dr. Blagosklonny, or any others for that matter, the correct dosing protocol for any one person. Taking some rapamycin is better than taking none in my opinion.
I only test during the period I am not taking rapamycin, usually 4 to 5 days after my last dose.
On high doses of rapamycin, my Hba1c and apoB were higher than normal. On my present dosage schedule, they have returned to normal.
Yes, but only if you are comparing the same weekly dosing schedules…
What we don’t know for sure is if you keep the same blood levels (e.g. 5ng/ML) for the same period of time (i.e. comparing apples to apples) I don’t know whether the amount of time it takes to start to see mTORC2 inhibition is any different.
Am I understanding correctly that Rapa doesn’t actually inhibit the action of mtorc2, but rather prevents new mtorc2 synthesis. Thus, it would take some time before a negative impact was seen.
Whether a break is needed or not depends on how high your dose is and how frequently you take it as well as on your individual response. If you take very high doses frequently you’re likely to benefit for breaks, but if you reduce either the frequency or dose sufficiently you will arrive at a point where you won’t need a break. Where the sweet spot is is hard to say and somewhat of a guess work but there are ways to gauge where you stand. I think there is no need to do complicated calculation of animal doses and concentrations to get good clues here. It’s much easier to simply measure your insulin sensitivity and your blood lipids before and after taking rapamycin for at least a month. Worsening of either of these parameters is a proxy for mTORC2 inhibition. If insulin sensitivity and blood lipids don’t significantly change, chances are you don’t need breaks. If on the other hand they get worse you likely either need to add breaks, or to simply reduce the dose or the frequency of dosing, then repeat the blood tests to see where you stand.
Btw, I find it a bit strange that some authors are taking rapamycin for 5 weeks on and then 8 weeks off. That comes out at 5 doses in 13 weeks or roughly one dose every 18 days. If the goal is to prevent mTORC2 inhibition they might as well just take a dose every 18 days instead of taking it for 5 weeks on and 8 weeks off. If 8 weeks off would be enough to restore mTORC2 from 5 weeks on, then you probably would never get much mTORC2 inhibition if you just took a dose every 18 days. 5 weeks on and 8 weeks off is IMO a bit like taking too much for 5 weeks and then taking a break for 8 weeks to fix it and then repeat.
@KarlT That is my understanding as well. Here is the quote from the paper.
“Although mTORC2 is not acutely inhibited by rapamycin, subsequent studies have shown that mTORC2 is inhibited in cell culture as well as in vivo in mice when exposed to high concentrations of rapamycin for a prolonged period of time, most probably due to the sequestration of free mTOR by rapamycin so that it is unavailable for incorporation into mTORC2 (refs. 17,32).”
@Olafurpall I get the feeling that some of the information shared online is posturing in response to or in avoidance of criticism for being too aggressive or wishful thinking about rapamycin. Some of these people have to be careful about their reputation. It makes the situation for people like us all the more challenging to figure out. Perhaps I’m wrong…
It would seem then that it might be better to take an isolated large dose rather than taking a lower daily dose that could over time wipe out a lot of mtorc2?
It would seem fairly easy to determine if your dose of Rapa is too high by checking glucose and apoB.
But how do you determine if dose is too low?
There are two leading experts taking low daily doses per my tracking. Meanwhile, most of the maintenance medication in practice is that once a chronic situation is stabilized, then it is a low daily dose for maintenance. Prednisone is one of them.
I am looking for proxies because it is very inconvenient for me to have my rapamycin levels tested because the ordering sites for rapamycin testing don’t have an association with Quest Labs.
“It’s much easier to simply measure your insulin sensitivity and your blood lipids before and after taking rapamycin for at least a month. Worsening of either of these parameters is a proxy for mTORC2 inhibition. If insulin sensitivity and blood lipids don’t significantly change, chances are you don’t need breaks”
Could you expand your thoughts on this? I am currently taking 1mg/daily for 7 days then 7 days off. No science behind this, just my own experience over the last ~2yrs of titrating down from 20mg/weekly.
Latest results ~1 week ago
HEMOGLOBIN A1 c= 5.6 Borderline
APOLIPOPROTEIN B = 71 ml/dL Good
LIPOPROTEIN (a) = <10 ml/dL (good genes)
I believe I am getting mTORC2 suppression because wounds, mosquito bites, etc., are slower to heal than normal.
Do you think an insulin test would be a better indicator than an HbA1c test?
When do you think would be the best time for me to be tested given my dosing schedule?
Right. What should rapamycin do? What impact should it have if the dose is high enough? Is any sign of restoration of function a sufficient signal? If no benefit is seen after x months, then the dose is too low?
Its interesting… I was asking people at the Longevity Summit at the Buck Institute last December about this (glucose and lipid disregulation) as possible biomarkers of mTORC2 inhibition. Tim Peterson (formerly in Sabatini Lab at MIT working on MTOR) said he did think that these might be a reasonable proxy for mTORC2 inhibition. Matt Kaeberlein disagreed and said he didn’t agree, and didn’t think they are necessarily a good proxy for it. Unfortunately I can’t recall the rationale for Matt’s thinking on this.
I think some people are affected by glucose and lipid dysregulation more than others. It’s dependent on biology and a host of other factors (diet, exercise, medications, etc.) I have both glucose and lipid dysregulation after taking 2 mg + GFJ pushing me into barely high areas on both (102 ApoB and 5.7 HBA1c). My father, who doesn’t take Rapamycin had 108 ApoB and 5.6 HBA1c. But we’re both taking Metformin. He takes 1 g and I take 500 mg daily. He fasts (OMAD). Since our scores are similar does it mean we have affected our MTORc1+2 the same?
Probably not.
So, blood biomarkers are good to know when you’re going off the rails, but they have to be viewed from the perspective of the whole - diet, sleep, supplement stacks, meds, Rapa, etc… It could be the Rapa you’re taking or it could be the McDonald’s hamburgers you’ve been binge eating with fries and Coke while watching the Late Late Show.
The question is whether your dose is too high for you since you get side effects. You could probably knock those side effects down with separate interventions but is that the right thing to do? I’m not suggesting you do anything. I’m just trying to understand how to use this sort of information.
I do not seem to get higher LDL-C or glucose but I have been taking medications for those issues pre-rapa. Perhaps I’m missing a clue about rapa. Or, if I’m not having symptoms of too high a dose, I could increase my dose to seek some measurable benefit from rapa. It’s an interesting question.
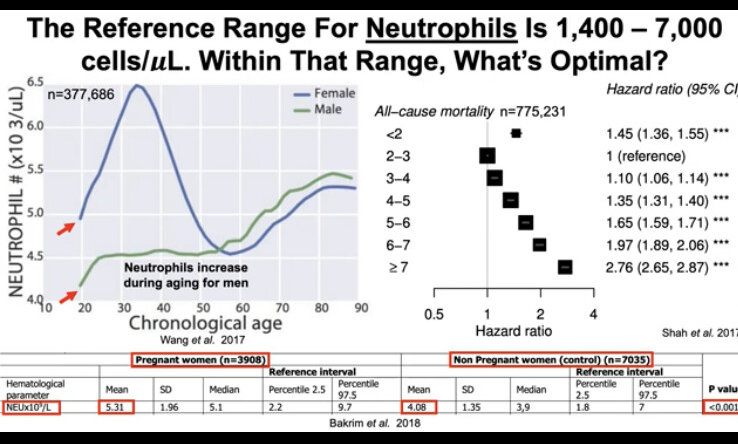
What is the relationship between apoB and Rapa? I am confused here, do you mean Rapa might increase apoB? given that a lot of people tracking apoB here, what is your trend on apoB since started Rapa? After 3 months on a mostly low daily dose (1mg), I have not seen glucose change but a significant drop in lipids which I contribute to statin. There is a drop in neutrophils from 3.5 to 2.5 which is still above the normal range but something I will be watching for.