@Olafurpall I get the feeling that some of the information shared online is posturing in response to or in avoidance of criticism for being too aggressive or wishful thinking about rapamycin. Some of these people have to be careful about their reputation. It makes the situation for people like us all the more challenging to figure out. Perhaps I’m wrong…
4 Likes
It would seem then that it might be better to take an isolated large dose rather than taking a lower daily dose that could over time wipe out a lot of mtorc2?
It would seem fairly easy to determine if your dose of Rapa is too high by checking glucose and apoB.
But how do you determine if dose is too low?
2 Likes
There may be a little confusion here, as Dr Attia in the past had said 8 weeks on, then 5 weeks off. I think he has since changed.
And my apologies to everyone for posting so many times here.
4 Likes
There are two leading experts taking low daily doses per my tracking. Meanwhile, most of the maintenance medication in practice is that once a chronic situation is stabilized, then it is a low daily dose for maintenance. Prednisone is one of them.
2 Likes
my recollection is that Peter Attia now is taking a weekly dose with no break.
4 Likes
Thanks for contributing your expertise.
I am looking for proxies because it is very inconvenient for me to have my rapamycin levels tested because the ordering sites for rapamycin testing don’t have an association with Quest Labs.
“It’s much easier to simply measure your insulin sensitivity and your blood lipids before and after taking rapamycin for at least a month. Worsening of either of these parameters is a proxy for mTORC2 inhibition. If insulin sensitivity and blood lipids don’t significantly change, chances are you don’t need breaks”
Could you expand your thoughts on this? I am currently taking 1mg/daily for 7 days then 7 days off. No science behind this, just my own experience over the last ~2yrs of titrating down from 20mg/weekly.
Latest results ~1 week ago
HEMOGLOBIN A1 c= 5.6 Borderline
APOLIPOPROTEIN B = 71 ml/dL Good
LIPOPROTEIN (a) = <10 ml/dL (good genes)
I believe I am getting mTORC2 suppression because wounds, mosquito bites, etc., are slower to heal than normal.
Do you think an insulin test would be a better indicator than an HbA1c test?
When do you think would be the best time for me to be tested given my dosing schedule?
4 Likes
Right. What should rapamycin do? What impact should it have if the dose is high enough? Is any sign of restoration of function a sufficient signal? If no benefit is seen after x months, then the dose is too low?
Its interesting… I was asking people at the Longevity Summit at the Buck Institute last December about this (glucose and lipid disregulation) as possible biomarkers of mTORC2 inhibition. Tim Peterson (formerly in Sabatini Lab at MIT working on MTOR) said he did think that these might be a reasonable proxy for mTORC2 inhibition. Matt Kaeberlein disagreed and said he didn’t agree, and didn’t think they are necessarily a good proxy for it. Unfortunately I can’t recall the rationale for Matt’s thinking on this.
6 Likes
I think some people are affected by glucose and lipid dysregulation more than others. It’s dependent on biology and a host of other factors (diet, exercise, medications, etc.) I have both glucose and lipid dysregulation after taking 2 mg + GFJ pushing me into barely high areas on both (102 ApoB and 5.7 HBA1c). My father, who doesn’t take Rapamycin had 108 ApoB and 5.6 HBA1c. But we’re both taking Metformin. He takes 1 g and I take 500 mg daily. He fasts (OMAD). Since our scores are similar does it mean we have affected our MTORc1+2 the same?
Probably not.
So, blood biomarkers are good to know when you’re going off the rails, but they have to be viewed from the perspective of the whole - diet, sleep, supplement stacks, meds, Rapa, etc… It could be the Rapa you’re taking or it could be the McDonald’s hamburgers you’ve been binge eating with fries and Coke while watching the Late Late Show.
7 Likes
The question is whether your dose is too high for you since you get side effects. You could probably knock those side effects down with separate interventions but is that the right thing to do? I’m not suggesting you do anything. I’m just trying to understand how to use this sort of information.
I do not seem to get higher LDL-C or glucose but I have been taking medications for those issues pre-rapa. Perhaps I’m missing a clue about rapa. Or, if I’m not having symptoms of too high a dose, I could increase my dose to seek some measurable benefit from rapa. It’s an interesting question.
3 Likes
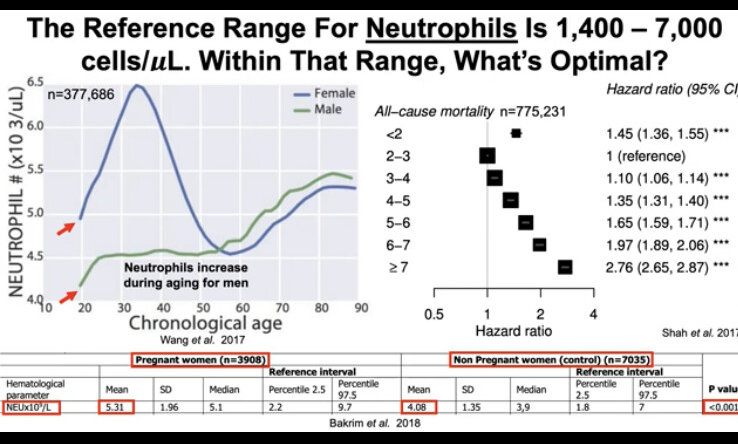
What is the relationship between apoB and Rapa? I am confused here, do you mean Rapa might increase apoB? given that a lot of people tracking apoB here, what is your trend on apoB since started Rapa? After 3 months on a mostly low daily dose (1mg), I have not seen glucose change but a significant drop in lipids which I contribute to statin. There is a drop in neutrophils from 3.5 to 2.5 which is still above the normal range but something I will be watching for.
2 Likes
Still, searching for that sweet spot. I have been doing 1 mg/day for 7 days and 7 days off.
I am still having trouble keeping my glucose below the high normal range.
Currently, I am taking 500 mg of metformin with rapamycin, a 50 mg acarbose tablets
before dinner. Also, I just added Linagliptin 5mg tablets four days ago morning and evening. “Linagliptin helps to control blood sugar levels by increasing substances in the body that make the pancreas release more insulin.” It is also sometimes combined with metformin in a single pill. So, far I have seen zero effect. Maybe it is still too soon to tell or I need to increase the dose. I have tried Jardiance Empagliflozin, also to no noticeable effect. Perhaps it is just because I am old.
The only insulin-sensitizing drugs that I can find have serious side effects and most of them have been banned in some countries.
So, my next plan is to reduce my rapamycin intake to 1 mg/day for 5 days then 9 days off.
I prefer to try this rather than increase my anti-diabetic drug intake.
As I have commented before: I don’t believe it is okay to have markers outside of the normal range even if you are taking rapamycin. Specifically, I believe that blood glucose should not be above normal. Glycation, from my readings, appears to be one of the most important things to reduce to prolong life span"
"Glycation, a deleterious form of post-translational modification of macromolecules has been linked to diseases such as diabetes, cataract, Alzheimer’s, dialysis related amyloidosis (DRA), atherosclerosis and Parkinson’s as well as physiological aging
“Hyperglycemia increases the glycation process, and is especially apparent in insulin independent tissues such as red blood cells, peripheral nerve tissue cells, endothelial cells, eye lens cells, and kidney cells”
“There is evidence to indicate that controlling hyperglycemia by antidiabetic biguanides prolongs life span in experimental animals. Caloric restriction, which appears to prolong life span by bringing about mild hypoglycemia and increased insulin sensitivity further strengthens the idea that glucose via glycation is the primary damaging molecule.”
7 Likes
1 mg/day for 5 days then 9 days off, that’s exactly my dosage at the moment. So far, with this schedule, I’m feeling better and at the last blood test, my kidney function recovered (that was my main problem with weekly pulse dosing). Blood sugar levels are better too, but they’ve never been borderline. I’m younger (52), but I have other health problems, particularly heart problems
9 Likes
Hello everyone, newbie here. I watched an interview with Dr. Kaeberlein in which he mentioned taking it once weekly for 12 weeks. It’s on YouTube. Also, I guess it depends on each person’s goals. Younger women with infertility issues are told to use it for a few weeks to improve oocyte quality, but stop when trying to conceive for several reasons. From my understanding, Dr. Kaeberlein got all he needed from Rapa in 12 weeks, so he cycles. I just started back in August, and I’m at 3mg/week, and I’m hoping it’s enough for a 5ft, 109 lbs person. I’m considering doing the 12 week cycle suggested by Dr. Kaeberlein. I have a large number of Bosniak type II cysts in my kidneys, 1 nodule in my thyroid, 2 cysts in my liver, and I have medium size uterine fibroids, so I’m actually taking it in hopes that by decreasing mTOR may help keep my cysts from increasing in both volume and also in number. I just hope I’m on the right track.
7 Likes
That’s about my size (5’1/103) and I’ve been taking 3mg/weekly fwiw.
3 Likes
2 Likes
That was off Rapa? On any Metformin or other glucose lowering medication?
Yes, that was off rapa, but I have been taking metformin for many years as it was noted long ago to possibly have life extension properties.