I have been wanting to have this discussion in the forum, thank you!
It’s all guesswork. The theory is that you don’t want to impede mTORC2 so you want it to go to zero before re-up. Blagosklonny has said it’s 50 to 50 for either taking weekly or daily, for instance. And he disputes that mTORC2 is inhibited (said just a few cell lines). And there is one expert who is taking 1mg daily. Peter Attia is on weekly one dose. What made you decide to take rapa and how’s going so far? What else you are taking for what purposes if you don’t mind sharing?
How much rapamycin inhibits mTORC2 is still up for debate.
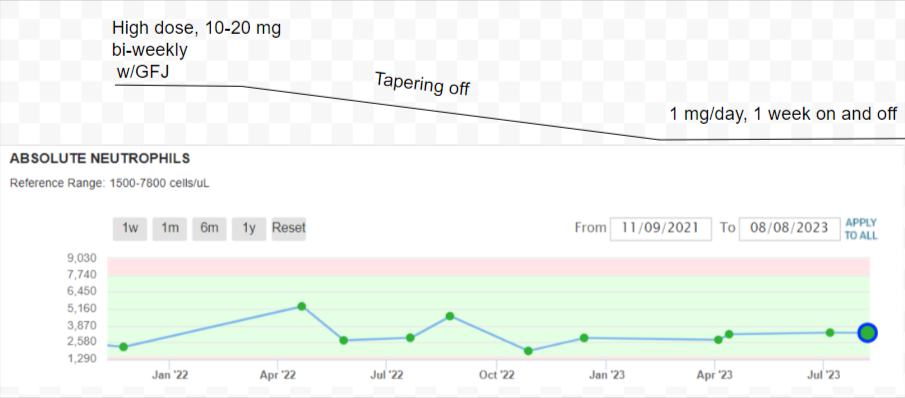
When I was taking high doses, up to 20mg w/GFJ, the only thing I experienced other than diarrhea, was a little slower wound healing and some thinning of my fingernails. I am 82, so you would think my immune system wouldn’t be as robust as a younger person’s. In the almost two years that I have been taking rapamycin, I have had no illnesses, colds, flu, or tested positive for COVID-19, etc.
I think major depression of mTOR2 from the doses that members are taking is unlikely.
But, that is just my opinion from reading various papers. I have no medical background.
I think you want either frequent very low dosing (think 1/2 to 1 mg per day range, depending on weight) or (and this is the much more common approach) pulsed weekly, or every two weeks… much higher dosing… somewhere between 3mg for light/more sensitive people to 20mg every two weeks or so, seems to be the range that is working with people.
I don’t think I’ve seen any evidence to suggest that mTORC2 inhibition is a positive thing for longevity. A number of studies suggesting increased mTORC2 levels might be helpful for longevity.
In fact, this recent research has got me more interested in fasting simultaneous to rapamycin use, as it seems that the fasting could boost mTORC2 while you’re suppressing mTORC1 with rapamycin, which seems to me might be the optimal approach:
Since we know rapamycin suppressing neutrophil to some degree, why don’t we use the range of neutrophil as a practical indication of whether you are on the right dosing regimen or not? Neutrophil is an innate immunity response. @RapAdmin@desertshores
I start on dosing with a hypothesis as to the mechanism we are trying to operate. I think that mechanism is improving the ATP/O efficiency of mitochondria via a route of encouraging mitophagy followed by some mitochondrial fission.
Hence there is a question as to how frequently do we want this to happen. I would personally think that it is not essential for it to happen every week or every fortnight. One would assume there is a stochastic element to this as well. Hence as a consequence of mTORC1 inhibition a proportion of cells (higher than otherwise) get some BECLIN1 created and this kicks off mitophagy.
Hence my approach which differs from everyone else. I look every so often to have a period when I am encouraging mitophagy. Although when I stabilise (I was on holiday, I had a gig yesterday at a beer festival and I have been attending another festival Friday, Saturday and Sunday, hence I am not fasting although still reserving carbs to alcohol consumption) I will probably reinstate two fasting days a week. Probably once a month I will take Rapamycin on one of those days.
There is an interesting, but complex protocol on Longecity about mitochondrial fission and fusion based around C60, but it looks to potentially have hazards so I wish to study that as an additional technique for improving mitochondria. (when I have got through all of my other ideas)
I hypothesise that because BECLN1 is a long gene it probably requires a high level of acetyl-CoA and also a goodly quantity of ATP to be available to enable the cell to kick off autophagy. Hence I intend thinking carefully about how to achieve this. (It it is at all possible).
I was referring specifically to the cycling schedule which was the original poster’s issue NOT to anything and everything else about rapamycin such as dosage etc. even though it may relate in some sense or order to other aspects.
@dan_hayes you are correct. Nothing wrong with your doubts. Anyone who thinks they know the correct dosing system at this point in time, is on the wrong part of the Dunning-Kruger curve.
how do we measure impact on the GI system? I noticed that I lost some belly fat, but no GI side effects except the product of my bowel movement is drier
I am not sure what you have in mind. Just looking at my neutrophil history, I see no obvious correlation between my rapamycin doses and neutrophile percentage. If rapamycin suppresses neutrophils, it must be for a very short time and does not show up on blood tests. There are probably too many other factors that affect neutrophils for it to be a good indicator:
“Factors that can increase neutrophil levels include Infection, Inflammation, Stress, and Vigorous exercise.”
Over the period of almost two years, I have tried various dosing protocols while measuring my blood work and noting the side effects they had. In a nutshell, high doses screwed up my health markers, specifically lipids and glucose. High doses with GFJ caused diarrhea and a couple of of nights of tossing and turning during my sleep.
I have done the opposite of what most people do. I have titrated down from a large dose.
Quoting from a Dr. Blagosklonny paper:
“For antiaging purposes, however, rapamycin may be used either intermittently (e.g., once a week) or at low daily doses and can be discontinued if any unpleasant effects occur.”
At a 5 to 10 mg weekly pulse dosing of rapamycin dosing with EVOO, I was still experiencing sleep disturbances on the first day even though I took the dose early in the morning.
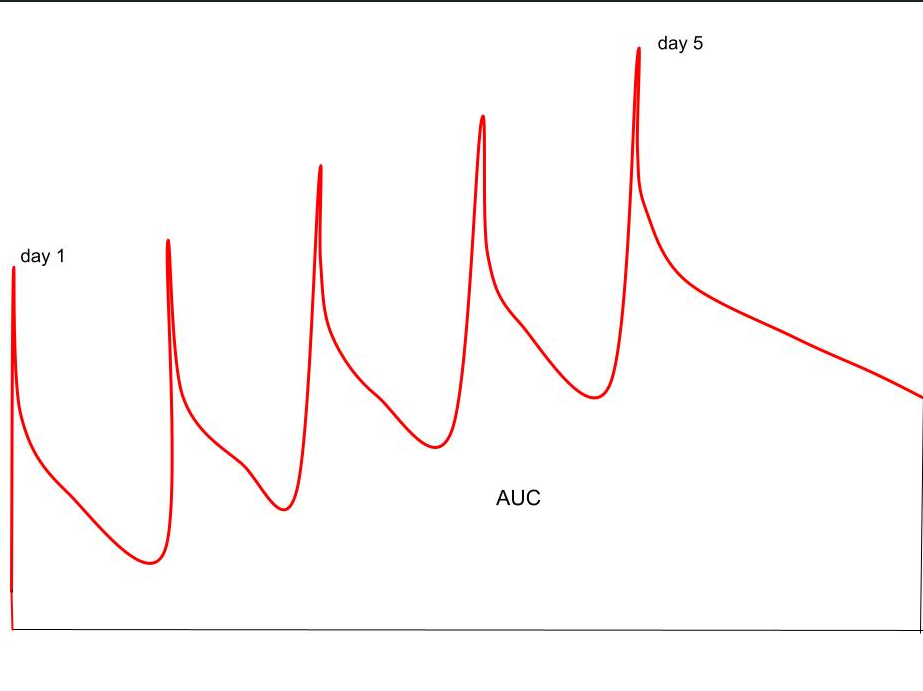
At 1 mg daily for seven days on, and seven days off, all of my blood markers are back in the normal range, even though the half-life of rapamycin would suggest that I get a larger AUC than a weekly pulse dose of the same amount.
This chart furnished courtesy of another member of the forum, sorry, I don’t remember who, shows a predicted 5-day schedule.
Oddly, on this schedule, I feel no side effects and feel no differently on days on than days off.