Waist size as a reflection of both insulin resistance and inflammation may be the most important biomarker of them all. A risk for virtually all age related diseases. Keep the height/ waist ratio in inches under 0.5 if possible.
Some people just can’t do it with diet/ exercise alone. For that group we’ve had remarkable success with semaglutide. Much better than anticipated.
Waist size is HIGHLY implicated, 100%. Metabolic Syndrome.
Estimated Life-Years Gained Free of New or Recurrent Major Cardiovascular Events With the
Addition of Semaglutide to Standard of Care in People With Type 2 Diabetes and High
Cardiovascular Risk
“Glucagon-like peptide 1 receptor agonists (GLP-1 RAs) are a class of highly effective blood glucose–lowering medications that provide cardiovascular benefit alongside improved glycemic control and weight loss (8). GLP-1 RAs are recommended for people with T2D and high cardiovascular risk in several recent guidelines (9–12).”
6480 persons, T2D at high risk of CVD
BMI 30+, hbA1C 8.4
But wait, the cohort LDL is only 85 mg/dL, TC only 166? Yet their TG is 183 mg/dL.
@rivasp12 When you say “remarkable success”, you mean weight loss/waistline?
These drugs work on “glucose control”, yet they purportedly lower CVD risk? How can that be if LDL mediated?
Yes. Semaglutide at 1 mg per week is the glucose management dose but the FDA approved it at 2.4 mg’s for weight management about 2 years ago.
We’re seeing 15-22% weight reductions. Very surprising actually.
We’ve now treated over 500 people.
Great YouTube discussion between these guys. Clearly we don’t want to claim that CVD should only be prevented/managed via apoB or LDL, and at the same time we don’t want to completely ignore metabolic health. Both are incredibly important.
Both make some good points, although the surgeon seems outmatched when it comes to the primary interviewer’s mastery of the facts.
I can definitely appreciate the surgeon’s primary point that there are docs out there who just “treat the LDL” and ignore the rest. My former cardiologist is one – he just told me to get LDL particles as low as possible, NO mention whatsoever of exercise, diet, abdominal fat loss, etc. The reasons behind this are multiple, but in the end probably due to time constraints. A discussion with a patient about diet and exercise could go on for an hour (depending on the pt’s preconceived notions and what he’s willing or not willing to do), meanwhile the waiting room has other patients waiting to see the health care provider. There’s just not enough time to do it. Much easier to just prescribe the med(s) and send the patient on his way.
multiple, but in the end probably due to time constraints. A discussion with a patient about diet and exercise could go on for an hour (depending on the pt’s preconceived notions and what he’s willing or
It’s also famously difficult for people to lose weight & keep it off. A discussion with a doctor, no matter how long it takes, isn’t likely to be enough to make a change.
It’s easy for people to learn that lowering weight, doing exercise, etc, are good for health. It’s hard to make it happen. I know more than a few people who want to do this, lose 10 or 15 pounds, gain it back & so on. I’m sure everyone on this list knows people like that, possibly ones that look back from the bathroom mirror.
Really love this information, thanks.
I could not find anywhere the amount of supplementation, it’s a meta study. Also supplements currently on Amazon are all over the place in amount and quality and quantity.
I’ve actually got a couple acres of aronia berries. It seemed like the thing to do at the time, but hard to find a market so we’ve been letting them drop off the last few years. I just pick what I can stand to eat.
In the YouTube video, if you fast forward to near the end at 1:01:40 it’s the point I’ve been making. It’s a good, concise summary. ApoB is an independent causal risk factor, even if a person is metabolically healthy and without other risk factors (which is rare).
(That was just meant as general reply, not specifically a reply to RapAdmin)
It’s interesting. The cardiologist sees patients referred from other doctors usually and often they have a history of cardiovascular disease, heart attacks, possibly angina. They’ll have an aggressive approach to lowering all risk factors.
In Internal Medicine we often see asymptomatics and otherwise healthy who have just lipids, or hypertension , sedentary lifestyle, etc. We tend to view these risks as additive in their effects and, unless the numbers are off the charts, we try behavior interventions first.
I very much look at family history and a parent with a heart attack or stroke under the age of 55 is a big red flag for me and I’ll be more aggressive.
Many, if not most , patients have an elevated BMI and especially an enlarged waist indicating visceral fat. It’s remarkable how fixing that tends to correct everything else.
It is true as mentioned that this can be a very difficult task and maintaining weight loss is particularly difficult. I’m starting to believe that the GLP-1’s like semaglutide are a real game changer in this regard. If we can get the weight off , we kill many birds with one stone .
Agreed, mainstream family docs pay lip service to lifestyle intervention, knowing full well almost none of their adult patients will heed their advice. Western society is a “sick care” model, not prevention. And they need to “turn and earn” patients vs lecturing; it’s a business after all.
But much simpler and more cynical, big pharma has the ACC/AHA, ergo their member docs, beholden to them and made statins the “standard of care” for lipids "management".
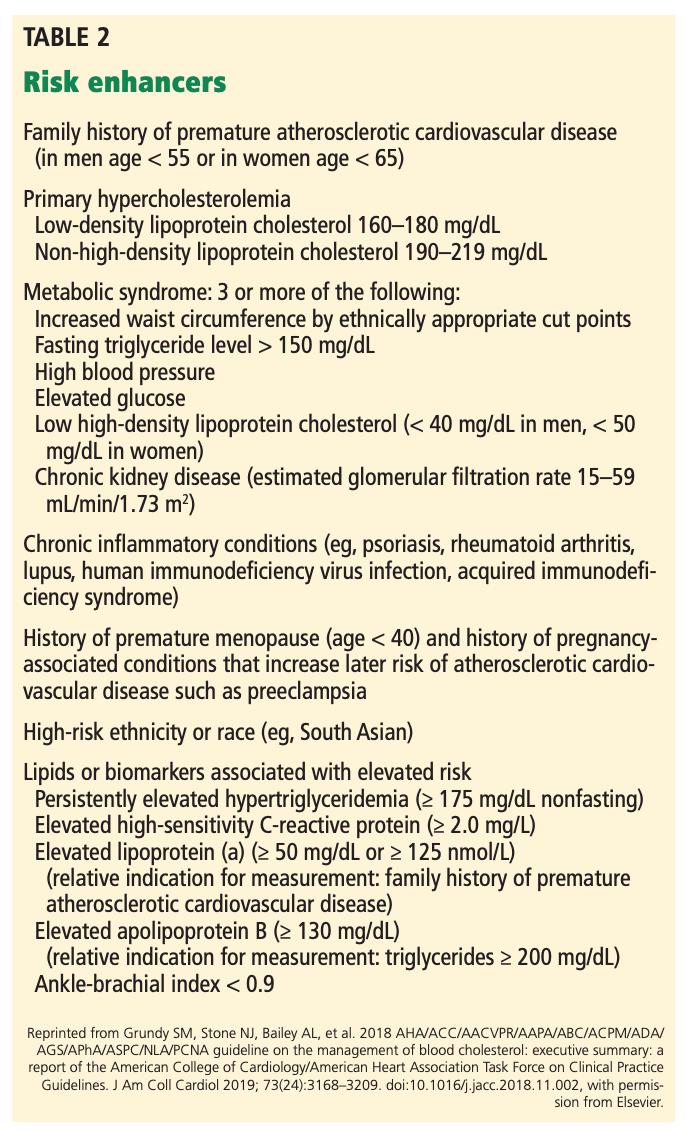
ACC/AHA lipid guidelines: Personalized care to prevent cardiovascular disease
" In addition to a heart-healthy lifestyle (which should be encouraged for all patients across their life course), statins are the foundation of lipid management."
Adults age 40–75 with LDL-C levels 70–189 mg/dL
Before starting statins, engage in clinician-patient risk discussion, evaluating risk factors, 10-year ASCVD risk, risk enhancers (Table 2), patient’s preference, costs, and adverse effects of statins
Use coronary artery calcium score to guide decision if risk is still unclear
@rivasp12 A recent paper on glucagon-like peptide 1 receptor agonists (GLP1-RAs) and CVD risk reduction.
Lipoproteins and Cardiovascular Disease: An Update on the Clinical Significance of Atherogenic Small, Dense LDL and New Therapeutical Options
"Because of reduced affinity to LDL receptor, sdLDL tends to circulate for a longer period in the blood stream. In addition, due to their distinctive physico-chemical composition, these LDL particles have greater arterial uptake and retention. They are able to penetrate into the vascular intima and are quickly transformed into oxidized LDL because of high susceptibility to oxidation.
Small, Dense LDL, Insulin Resistance and Diabetes. We are in the midst of an inexorable increase in the incidence of T2DM worldwide [32]. The atherogenic lipoprotein phenotype manifested by hypertriglyceridemia, low HDLcholesterol concentrations and elevated levels of sdLDL particles [3] is predominant lipid abnormality in subjects with insulin resistance, T2DM and the metabolic syndrome. The genesis of sdLDL is closely linked to the presence of hypertriglyceridaemia. In summary, the direct action of GLP1-RAs on sdLDL, as exemplified by liraglutide, is most likely due to their modulation of the pathophysiological alterations responsible for the proatherogenic activity of lipoprotein subfractions [51]. Of note, it may represent one of the key mechanisms by which GLP1-RAs are able to reduce cardiovascular events and mortality"
This is very interesting MAC. I wasn’t aware of the effects on sd LDL by
GLP-1’s. Very informative.
If you titrate up slowly with dosing, the side effects are pretty minimal.
The main issue, as always, is that we’re controlling glucose, lipids, and weight- but not actually curing any of it. They’re all chronic problems requiring chronic treatment.
Some massive LDL (580 mg/dL in A), TC (650 mg/dL in A) and apoB numbers. There is some serious energy intake and trafficking lipids in their veins.
I’ve always been on a “clean” plant fat based ketogenic diet (20% animal protein, 80% plant fat, majority MUFA/PUFA vs saturated), with very minimal amounts of animal and dairy fat (very lean cuts of meat, lean seafood).
My 6 yr average LDL and TC 139 mg/dl, and 217 mg/dL respectively. My last panel, TG was 52 mg/dL, HDL 77 mg/dL (TG/HDL 0.67).
This is interesting. So they followed over 800 women for 40 years to see what risk factors prevented them from getting to 85 years old. The strongest risks were smoking and physical inactivity. Of significance were obesity and not being married. No association with either lipids or BP.
Never knew that being unmarried was such a big death risk. Is it just a female thing? Men too? I’ve read that divorce is a greater mortality risk in men.