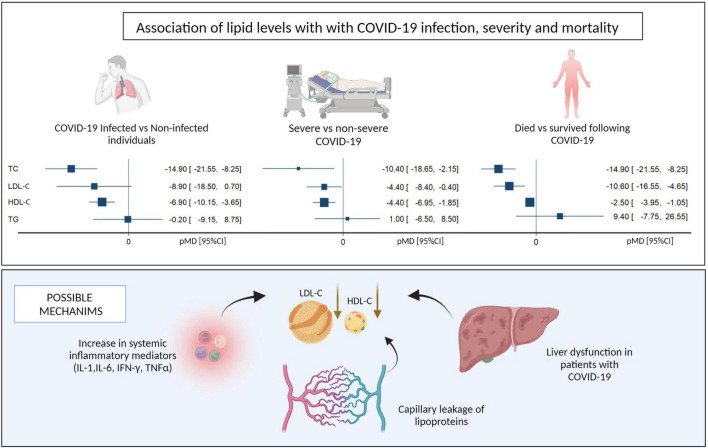
Another observational study which at first glance would appear to suggest that low LDL (and low HDL) cause more severe COVID. In fact, the proposed mechanisms are the other way around, that COVID/inflammation/liver damage causes decreased LDL and HDL.
This is the problem with observational studies that show increased mortality with lower LDL. If anyone can show me a study where LDL was pharmacologically lowered and then an increased rate of infections was seen, then that would be interesting. To my knowledge, that’s never been seen in the clinical studies with LDL lowering supplements or medications.
Brand spankin’ new video from Brad Stanfield MD, addressing/summarizing much of what we’ve been discussing/debating. The first part is just review, but keep listening…
Very little financial incentive to run that type of study. Besides, the argument would then just be that it’s some other variable and not the low lipids responsible for the infections.
Everything in biology seems U shaped.
Hyperglycemia bad
Hypoglycemia bad
High IGF- 1 and low IGF-1
High HDL bad
Low HDL bad
Too much mTOR
Too little mTOR
There’s no reason for lipids to be the exception. In general don’t overreact and don’t tinker too much with a finely evolved and complex physiological system that we poorly understand. We did that when we tried to raise HDL and watched people start to die of heart attacks.
There’s lots of studies now associating low LDL with overall mortality and even infections. Enough for me not get too extreme with it until we know what we’re doing.
More out of date doctors. This study from 2021 on patients with stable angina demonstrated that Triglycerides/ HDL was the most sensitive marker of progressive disease by the gold standard of angiography.
Just my non-scientific wondering on this subject ….
The body produces its own cholesterol for its uses/needs which is transported around with lipoproteins of various sorts, and it appears that one use is for helping to clear bad stuff out of the system.
Logically then LDL could be elevated when on a bad diet and all the while one is losing weight or benefitting from autophagy from whatever means etc.
As the liver then clears the LDL, I see nothing wrong with helping it if LDL is abnormally high if one doesn’t get side effects as a result. That said, one shouldn’t discourage the liver from being up to the job without help (Use it or lose it). Therefore, it might make sense to cycle LDL-c lowering drugs.
Once the body is at optimum weight and all the bad past damage that can be removed has gone, then assuming the food inputs are not bad then LDL should naturally lower itself and a properly functioning liver will do its job without help.
Maybe wishful thinking but to me it fits with both sides of this argument going on in this thread.
Unless I read the article wrong, the problem of this study is that the people are both old* and overweight. BMI +27.53 ± 3.60 from the cohort.
Plus a large percentage were already suffering from hypertension, diabetes etc.
Short-term rapamycin persistently improves cardiac function after cessation of treatment in aged male and female mice.
(University of Washington dissertation by Ellen Quarles)
This is a really interesting paper. It may explain why Matt K takes rapamycin for 10 weeks and then cycles off for a sustained period of time. It also seems to suggest that rapamycin may be effective against LV stiffening (For lack of a better word).
I’ve always been terrified by this study because the premise was that exercise after age 65 or so might be beneficial but would not affect cardiac plasticity. So the whole premise of the study was to look at healthy sedentary people 50-63 to judge the effect of exercise.
“ By contrast, if exercise training is started too late in life (e.g. after age 65 years), there may be little effect on LV stiffness as a result of a reduction of cardiac plasticity in sedentary, senior hearts (Fujimoto et al . 2010; Fujimoto et al . 2013).”
Interesting look at a 10 day water fast. Almost a 10 drop in weight and a steady loss of body fat accompanied by a drop in systolic blood pressure.
The LDL and ApoB went up by approximately 45%!
This is a similar effect I first encountered when I went on a ketogenic diet. My morning fasting glucose levels went way up. The ApoB didn’t go up much on TRF. It’s like when we are fasting the liver just keeps pumping out more glucose from the glycogen it is storing.
While I was on a ketogenic diet my lipids increased but were never out of the “normal” range.
On rapamycin, ApoB is the same but my lipids, especially triglycerides, increased well beyond the “normal” range.
I had my blood drawn on the morning I started a five day water fast and then blood work done 28 days later. Glucose went down substantially. LDL went down substantially. HDL up a little. Triglycerides down.
I suspect that during and immediately after a fast, the flood of free fatty acids released from fat storage has an acute effect on raising LDL/ApoB, which then normalizes after the fast ends and body the re-adapts to food, after which a longer-term decrease in ApoB, LDL is observed as long as fat loss is maintained.
Looks like that’s the case after reviewing the above paper posted by Rivasp12. Seems strange that they didn’t measure free fatty acids, since I think that’s the majority of what’s released into the blood during fasting rather than triacylglycerols (aka triglycerides).
Probably many more than that but I didn’t chase down all the references.
So when I got afib from (most likely) low magnesium and I was referred to the best heart doctor around. That clinic was very nice and so were all the members of his team. I asked what caused it and asked several specific questions about cause. He said it didn’t matter what I eat and never mentioned dental hygiene either. These papers aren’t brand new, they act like this is common knowlege, just going by the language in the papers. The bacteria cause the infection that starts the ball rolling.
Why don’t I get a test for my microbial burden at my next checkup? If it’s high then what do I do? Ozone?
As someone with both a degree in medicine as well as dentistry I think I can safely say that MDs are completely clueless about anything related oral health…
If you want your teeth to rot out of your mouth eat many small meals throughout the day with plenty of carbohydrates and fruits and what do doctors recommend…