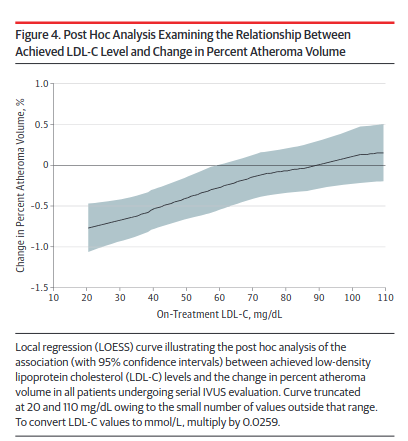
The percent of atheroma volume, or PAV, may be more accurate , and is significantly reduced with LDL < 90 with HDL >45. This may be a more realistic goal for primary prevention in the low risk person. This also is in line with studies that show a benefit of ApoB to ApoA 1 ratio of under 0.8. Shows that both have importance.
Keep an eye on bilirubin. A known side effect of pantethine is extended bleeding.
Thanks, I appreciate the heads-up. I will keep an eye on it. Oddly my bilirubin has gone down since I started taking it. Of course, I always have changing variables so I don’t attribute it to the pantethine.
And, as one would expect, pantethine and anticoagulant Pradaxa not a marriage made in heaven.
Started Pantethine July 11.
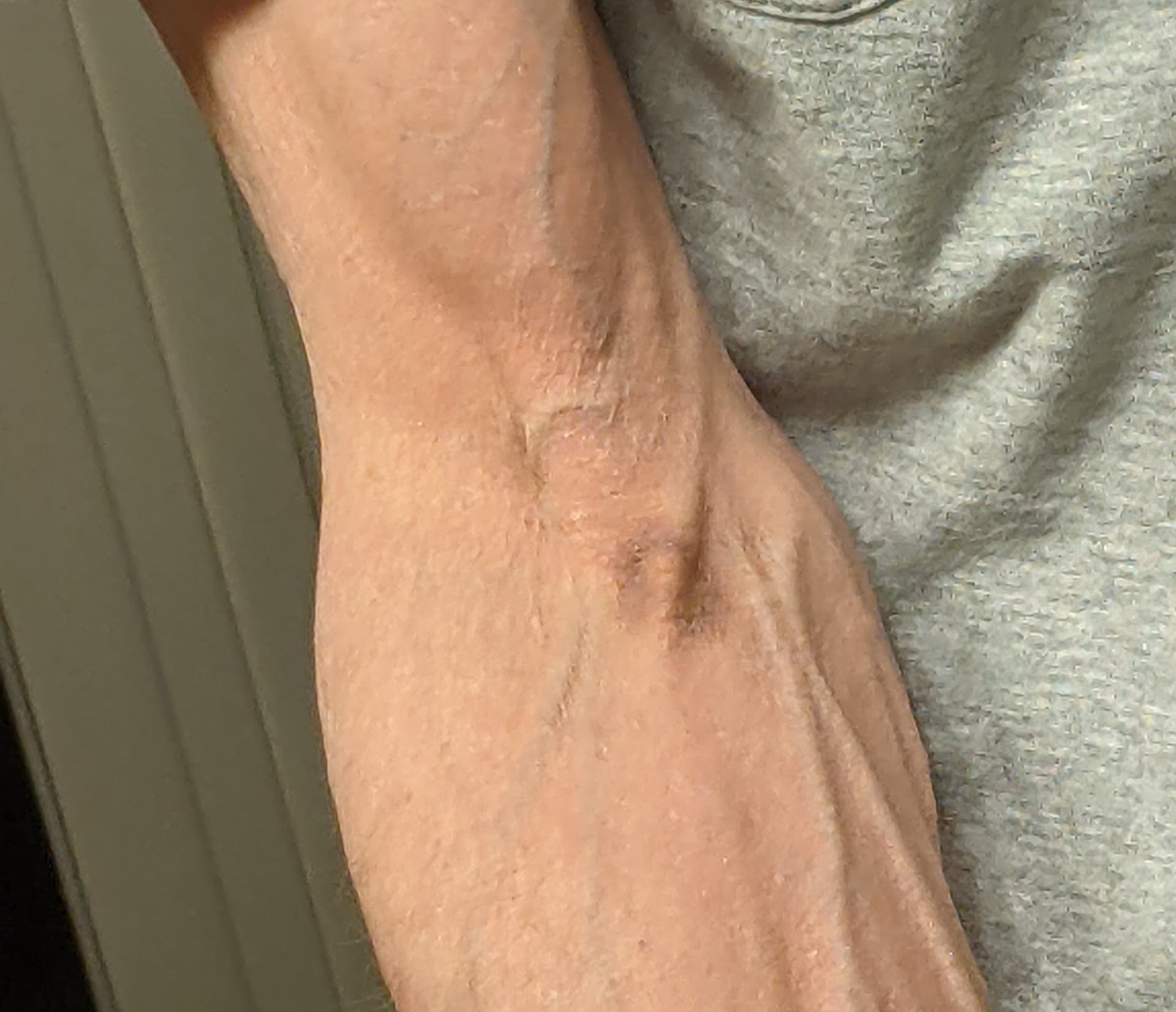
The first photo is from a blood draw three days ago. Sometimes I get a little bruising, but this time, the Ring Nebula.
Second and third are from today, where I got banged up a little while hiking. Has happened many times while on Pradaxa only. This outcome shows far more extensive bruising, relative to the severity of injury.
OTOH, got a record low apo-b reading from the ring nebula blood draw. I assume pantethine gets the credit.
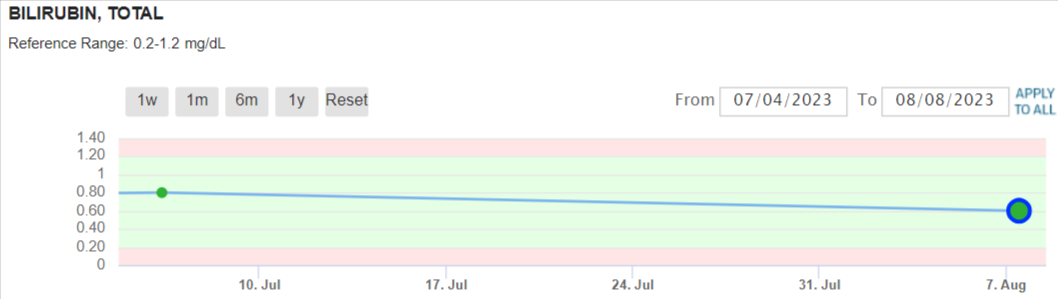
Bilirubin is .5, within normal range.


2 Likes
I don’t think it answers my question how many people have no progression at below <70 mg/dl vs. above.
Regarding lower levels, here’s the PCSK9 inhibitor study of Repatha showing a greater percent of people having regression from lowering from 90 mg/dl all the way to 35 mg/dl vs. placebo.
Evolocumab induced plaque regression in a greater percentage of patients than placebo (64.3% vs 47.3%; difference,17.0% [95% CI, 10.4% to 23.6%]; P < .001 for PAV and 61.5% vs 48.9%; difference, 12.5% [95% CI, 5.9% to 19.2%]; P < .001 for TAV)
In people with a baseline LDL of below 70 in this study, meaning what they started with before Repatha, more people also had a regression in plaques:
In patients with a baseline LDL-C level less than 70 mg/dL, post hoc analysis in the current trial demonstrated regression in PAV in more than 80% of patients with combination therapy.
But this study doesn’t answer the question how many had no progression.
Effect of Evolocumab on Progression of Coronary Disease in Statin-Treated Patients
The GLAGOV Randomized Clinical Trial
It’s worthwhile to note that it isn’t possible to reverse cardiovascular disease, so that’s why I am interested in which therapies or what LDL or apoB makes it so the disease doesn’t progress. Regression is all good, but it won’t regress plaques to 0…
2 Likes
I am a great fan of Pantethine, but think people should know the negative effects. This gives a good reason to stop taking it when you need more coagulation. I tend to take it when drinking (a lot at the moment because I am on holiday) I have managed to get my bilirubin down quite low, however.
As a later thought I think I should mention that one thing to be careful about (as with aspirin) is internal bleeding.
Citrate speeds up repair processes (by my experience) so that is a counter to the effect of Pantethine.
I don’t think anyone else has tested Citrate for its effect on repair, but if people are looking for a discrete experiment trying a short burst of citrate to get things repaired would be interesting, but first you need to make sure that your body can cope with multiple grams.
I thought i would provide a comparative photo. I am 63 and have a weekly blood draw. I use pantethine a lot but not every day. In the past year i have had over 44 blood draws from the same arm and one from the other. The last was 9 days ago. It repairs over a couple of days.

3 Likes
Hmm, of course at my age I have had too many blood draws to count. Sometimes, at all stages of my life, I have had bruising, sometimes not. I always attributed it to the skill of the phlebotomist drawing my blood. Do you usually have the same phlebotomist?
2 Likes
Labcorp personnel change frequently.
The bruise this time is at least 2x the size of any in recent memory.
I’m sure you considered the dosage? 2000 units is not one of the larger doses I’ve seen used in studies.
Each lab tends to have a different phlebotomist.
Since the absolute total mortality risk reduction in primary prevention of CVD is very modest with lipid lowering alone, it’s being suggested that raising tPA levels to combat clotting directly could solve this problem:
LDL not the be all, end all in heart disease, heart attacks and stroke (medicalxpress.com)
Nattokinase does just that. It increases levels of tPA. An RCT on nattokinase in low risk patients showed no significant benefit.
Nattokinase atherothrombotic prevention study: A randomized controlled trial - PubMed (nih.gov)
Low risk patients are just that- Low Risk- and it’s difficult to move the needle from low to lower, at least to any significant degree on absolute mortality rates.
6 Likes
I have problems with veins in my arms bc of frequent blood draws. Do you mean that Citrate alone helps to repair or in combination with Pantethine?
My personal experience is that grams of citrate helps with repair. However, I cannot guarantee anything. Pantethine potentially acts contrary to this. (in facilitating bleeding). That reminded me, however, to take some Pantethine and DHM. I played a gig today at a Beer festival and then went to a Folk Festival, but I had forgotten to take my anti (the bad effects of) alcohol regime of 2g of pantethine and 1g of DHM. Which I have now done.
IMO Citrate helps with repair, but Pantehine does not. However, be really careful with citrate as it can have side effects (see my previous posts).
2 Likes
The absolute risk reduction is only small because a) the absolute risk is small to begin with b) the studies are short and c) the patients in the studies were already exposed to apoB particles for decades. If you start early and treat aggressively, the absolute risk reduction could be huge.
That being said, I absolutely do agree that you can further decrease your risk by using anti-inflammatories like colchicine, blood pressure medication or other supplements that may help clear up existing plaque (vitamin k2, nattokinase).
2 Likes
Certainly some valid points. It would be great if we could identify and treat All risk factors at an early age, even poor sleep and stress. Same goes for cancer and they share many risks like obesity, sleep, stress, and smoking.
The practical problems there are immense , but it would definitely save millions of lives. One of the biggest hurdles is the feeling of immortality in the younger age groups.
6 Likes
so I have a spot just like that, slightly protruding whether I have had a blood draw in recent days or not. What does it mean? (the protruding)
I am not clear as to what you mean.
Could mean thrombophlebitis if you had frequent blood draws in that area, or, if not, it could be just your anatomy.
1 Like
There was a progression of the median coronary plaque volume (millimeters cubed) for each quartile of visceral fat for total plaque volume (upper left), NCP volume (lower left), and LD-NCP (lower right), although not for CP (upper right). CP, calcified plaque; LD-NCP, low-density noncalcified plaque; NCP, noncalcified plaque.
5 Likes
I still have not noticed anything from taking 15 pioglitazone, but if it moves fat from visceral to sub q then that would appear to be a good thing. It also eliminates glycated proteins. No side effects.