The one other thing is that statins can increase Lp(a). The general thinking is that the larger ApoB lowering of the statin still generates a net positive above the smaller Lp(a) increase.
But I’d still test Lp(a) before and after starting a statin and if the Lp(a) effect is large one might consider one is the cholesterol meds that are neutral (eg Eze) or positive (PCSK9i) on Lp(a) - or combine eg those two instead of combos with statins.
(I am very pro statins in general, just talking about the case where someone does not have optimal Lp(a))
@zazim - see above, perhaps consider Eze vs Statin on top of your PCSK9i)
As discussed in my last 3-4 posts above while this is a directionally correct, is not correct in the context of a dedicated health optimizer/bio hacker.
Besides the 4 ways Lp(a) test results can change that I discussed above, there is also lipid aphaeresis and some other implements, including, Niacin that lowers is (although we don’t not know if that also lowers bad outcomes).
Yes, even with an Lp(a) is in the upper 5%, they only represent about 10% of my circulating lipoproteins. There is a formula if you want to do the math based on your own scores. So, even though I don’t get the full effect of a statin, it is still very useful to treat with a statin.
I also highly recommend the Boston heart balance test. In my case It showed that Zetia would do nothing for me. (I had already started before I got the test. After two months, it reduced my LDL from 109 to 107.) This test is also helpful if you’re doing something wild like supplementing with plant sterols. They could help you or be incredibly harmful, depending on how you fare on this test.
My only fear is that these drugs will not initially be approved for primary care patients. I asked one of the doctors involved in one of the studies. The answer was we don’t know.
Once that happens, I will shift off of the PCSK9. Everyone was shocked that my insurance approved. I was prepared to pay out of pocket.
I would posit that even the most dedicated bio hacker would not find it valuable to retest. Obviously if you’re doing something like aphaeresis it would change, but absent that none of these other interventions are clinically relevant. For these trials to be successful, they will need a reduction of something like greater than 70%. If you test high, you are high, and there’s really nothing you can do about it for now other than optimize every other risk factor. Hence, my PCSK9 inhibitor.
From the last two data points there was enough data for my cardiologist and me to ask ourselves if it might be worth trying a full dose of Repatha instead of the half dose. (A half dose lowered my Lp(a) 25%). This is an experiment we are doing right now.
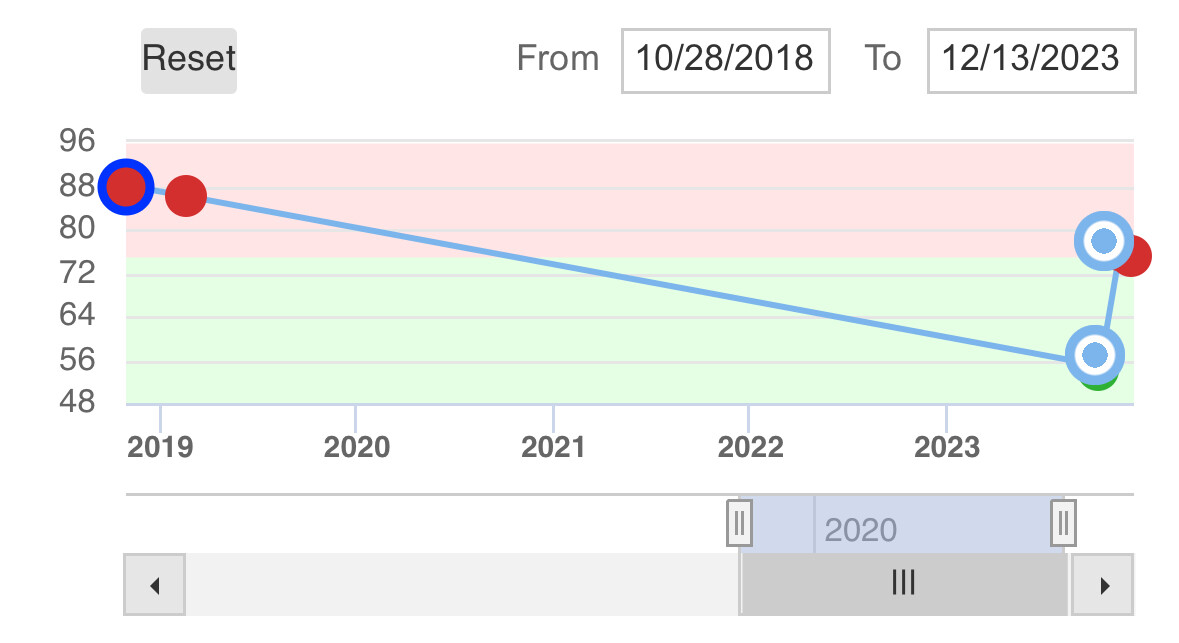
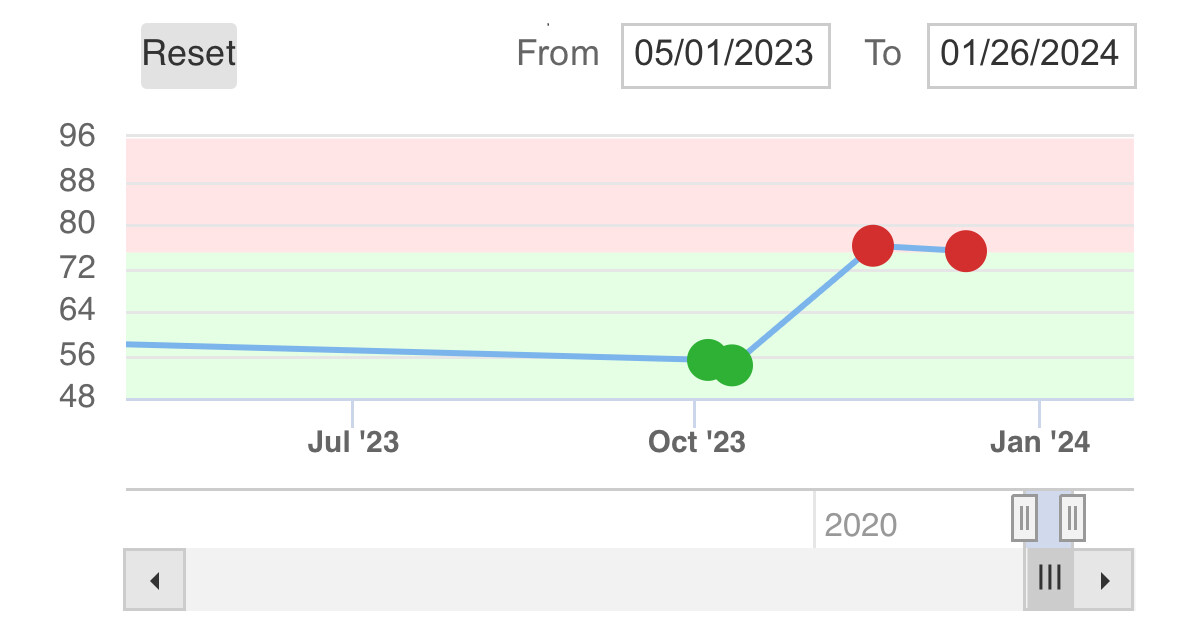
But what if the only Lp(a) blood test we took was the Quest Diagnostics one from October 2 or 6 2023 where the levels were ~55? Those were BOTH from a period when I had not been on PCSK9i or any cholesterol med for many months.
Either I had found some magical way to lower my Lp(a) via diet or exercise or supplemented that there were no know Lp(a) benefits from… or much more likely those two tests has testing errors.
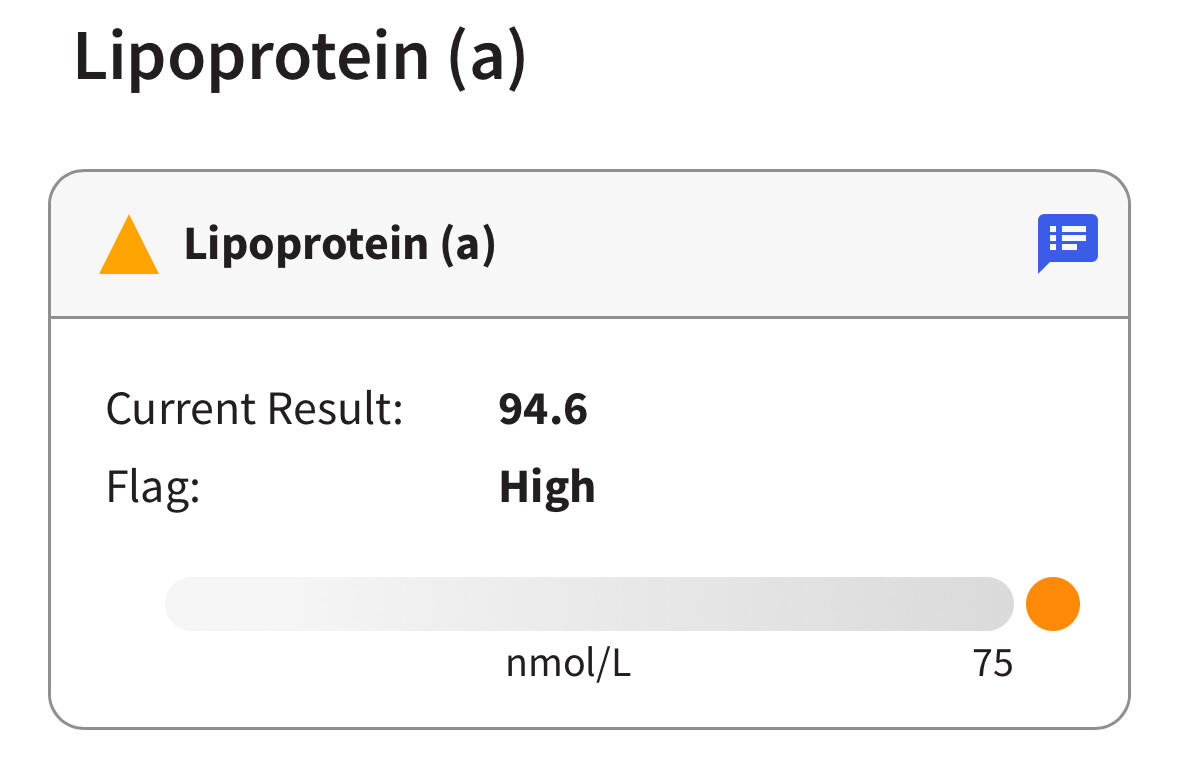
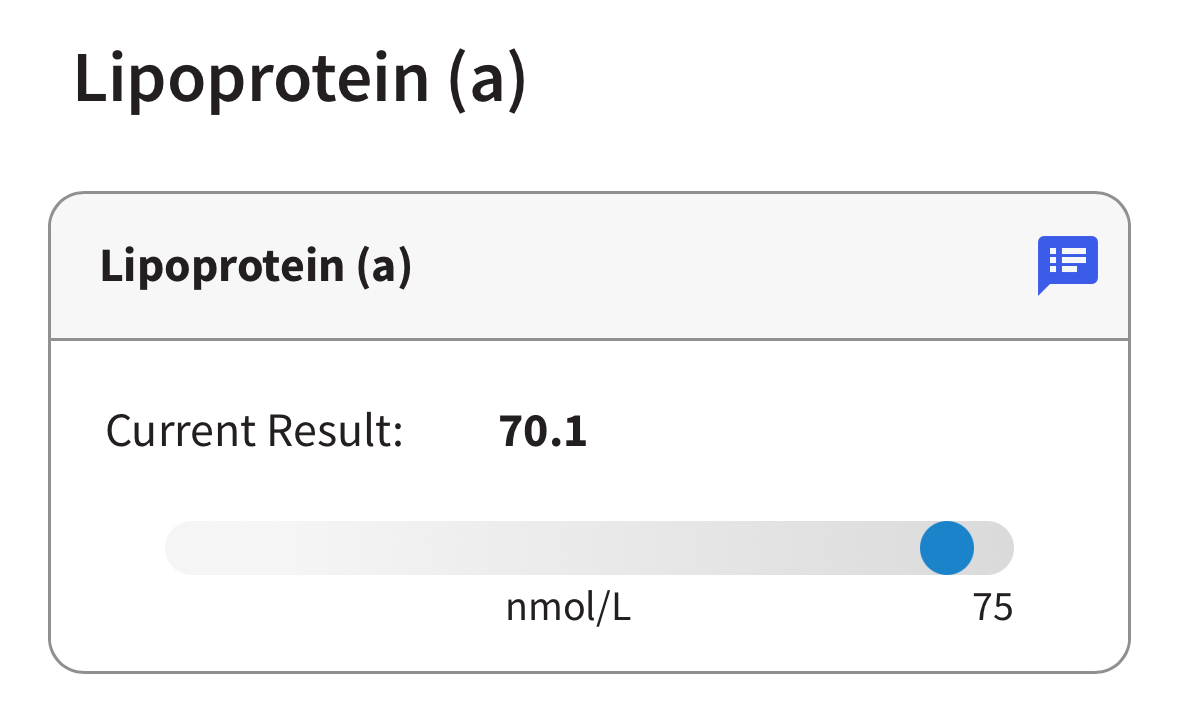
But if we only had one (or even both of those data points) and thought they was my baseline (a) we would be less concern and I may not have pushed for taking PCSK9i and (b) when we then looked at the Quest datapoints from when I was on PCSK9i in November and December at levels around 75 or so, we could have concluded based on data that PCSK9i increased my Lp(a) level by 35-40%….
Clearly when we see all the data points it’s almost certainly that I’m around 85-100 when on no medication, and it goes down by perhaps 25% to 70ish whenever I do decreases level PCSK9i.
This is just one example of why we should rely on more than one data point when gathering data to make decisions on.
There is always an error bar around any blood test, so you have to think about any one data point as being within a confidence interval that generally can be quite wide.
It seems that the Phase 2 data and pre-clinical data makes that very likely to be the case. The bigger question mark I think is was the disease outcome impacts will be from lowering it that much.
Only one of my labs tests for lp(a). I have glanced at this and it is quite low . I have not been recording it in my spreadsheet, but I could go through and see what variability it has if people would find that helpful. There is quite a bit of work in doing this, however, so I am not enthusiastic. Would people find it useful?
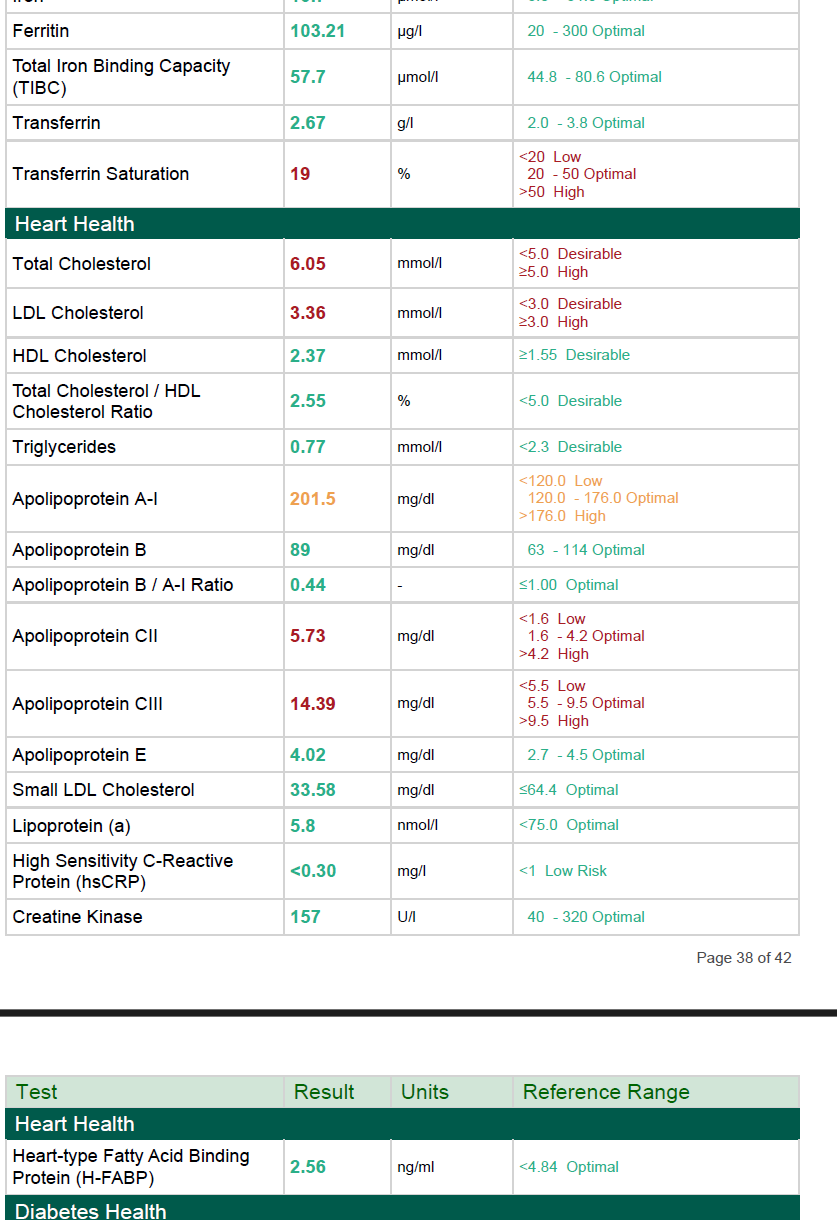
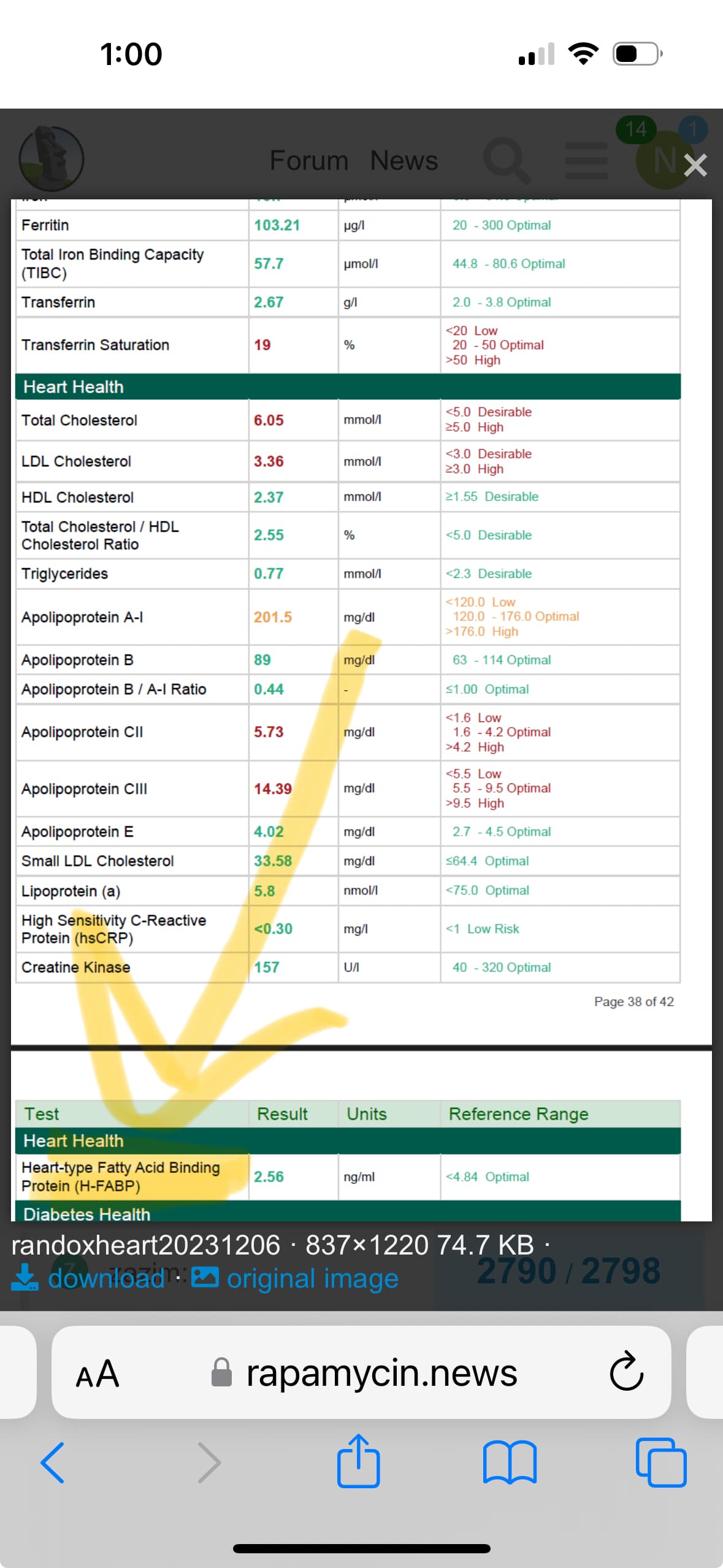
I will extract the page for curiosity. I don’t fast for the test and don’t worry about the LDL-C because it bounces around the Uk threshold which is 3 mmol/L.
I agree that we do not know what is clinically relevant, but a lot of the best guys in the world on Lp(a) to think that lowering in by 20-40% may be helpful and hence fight for PCSK9i for their patients. So I do not think you can say that it is not clinical relevant.
In fact as discussed on one of the Lp(a) threads on this forum you can see that there is clinical data that seem to show that PCSK9i are having benefits in people with higher Lp(a) that goes beyond the LDL lowering effects.
And where there is an option to avoid having Lp(a) up from statin use (in your case perhaps via Bempedoic Acid instead of statin given your cholesterol balance test and experience that Eze does not have any real impact for you) they often try that path out. So for that is a case where one might also want to measure Lp(a) changed - to understand whether the statin increased Lp(a) or not in a given individual.
This for me is the difference of precision medicine that a dedicated health optimizer/biohacker can pursue. I understand that most patients and physicians don’t have the energy or often cannot or do want to prioritize the time and/or resources to approach things this way.
Thanks John. From my perspective, given how low yours is it would probably be more interesting to see how much it bounced around with someone who has higher / more concerning levels.
I had a bad experience with Randox: when I got the results, my PTH was too high (8.5 pmol/L), while calcium and vitamin D were OK. I went to see my endocrinologist. He told me that I was the third person this month coming from Randox with an elevated PTH but normal calcium and vitamin D. He redid the test for all of us with an accredited lab, and they came back normal (4.6 pmol/L). So I’m afraid Randox is not reliable. Too bad because it’s the cheapest…
Since cardiovascular disease - and heart disease stroke alone - are the by far biggest killers and drivers of awful disability - in the western world, I think one has to see normal Apo B as one of one’s largest risks (even if healthy, exerciser, etc).
Not until you have optimal Apo B should you be satisfied if health and longevity optimization is your goal.
Especially in the context that there are powerful meds with side effects profiles that are good.
I not researched this. Most recently i have been working on getting my rhr and bp dpwn following a metabolic boost. I now am back to a hr just over 50, but with a higher stroke volume. I am curious about these figures, but they dont seem a priority.