And there may be risks to targeting extremely low ldl-c. I think it’s important to note that the Odyssey trial thought: “It is important to note that, although adverse consequences of very low LDL-C were not identified in these trials, the long-term effects of very low levels of LDL-C induced by PCSK9 inhibitors are unknown.”
The mendelian randomization studies also detect a negative re diabetes:
“In conclusion, genetic variants in PCSK9 that associate with lower concentrations of LDL cholesterol are also associated with a modestly higher risk of type 2 diabetes and with associated differences in measures of glycaemia and bodyweight”
My LDL dropped from 152 to 95 within 7 months on rosuvastatin 5mg, ezetimibe 10 mg + supplements. For the first time my cholesterol is normal, but CAC is elevated (almost 300 for coronary artery).
So as in my case, with a positive CAC, low dose statin is advisable to reduce risk. Hope you’re taking K2 and CoQ10 as well to minimize side effects. BTW - I’ve read that water soluble statins (like rosuvastatin) are less risky than fat soluble ones. Also consider taking Kyolic Aged Garlic and Nattokinase as well (look up the studies on PubMed).
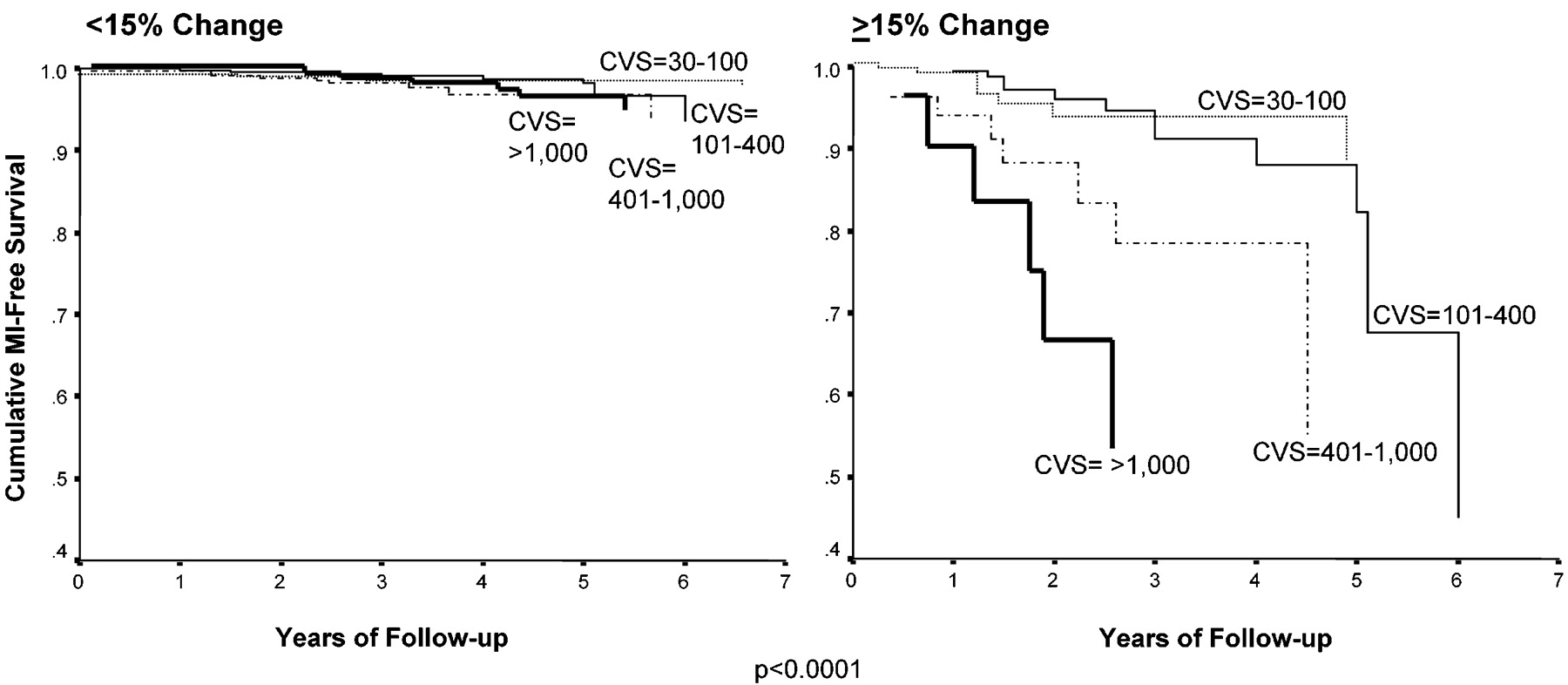
One interesting study on CAC showed that if we can reduce the growth of CAC to less than 15% year then our risk of an MI drops significantly, and approaches that of someone with a CAC=0. That’s a worthwhile target (though obviously you don’t want to be get tested every year because the radiation has its own risks). I plan to get a follow up test 3-4 years from now. Crossing my fingers! LOL
It may be true that the rate of progression varies and hence it is possible that it can be static. However, the underlying difficulty is having a system for measuring CAC that enables someone to track it without harm (or massive cost).
It may be possible to pick this sort of thing up from complex measurements of blood flow.
However, in the end I think there probably is a point where the absolute levels indicate more frequent measurement.
Yes, you’re right it may be more predictive without being useful for practical reasons.
I was also thinking that it would be helpful psychologically for people to know that, despite high CAC, if they could achieve low apo B / ldl-c then their risk is potentially much lower than most would believe. There’s nothing like a bit of hope!
It would be nice if we could have better systems of measurement. We would then be able to tell if a mixture of menaquinones, vitamin D and citrate can reverse it.
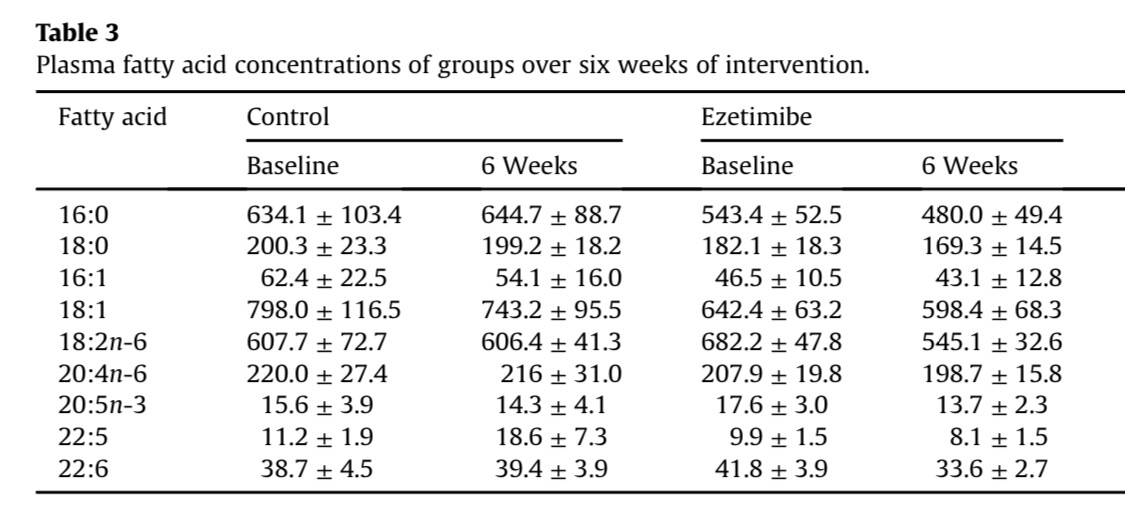
I just wanted to go back to this topic. Ezetimibe negatively impacts absorption of some omega 3 ,(ALA). And the benefit of ezetimibe is affected by EPA status - suggesting that it’s benefit might be negated by it’s negative impact on EPA absorption.
Does anyone have a view on this?
Given that omega 3 has benefits beyond atherosclerosis, blocking absorption is quite a cost.
Do you know if there is direct evidence on ezetimibe and DHA/EPA absorption? Either positive or negative?
The study i quoted relates to EPA. It suggests that if your EPA levels are good, then then the ldl-c benefit of ezetimibe is offset - suggesting that EPA absorption may be blocked.
Have you checked this study? It is small sample and statistically insignificant but there are some indications that ezetimibe affects absorption of omega 3.
Thank you, it is small, but persuasive for ALA. And I can’t quite see how ezetimibe would block ALA and not the other omega 3s (Dha and EPA).
I’m planning to experiment with micro dose ezetimibe - but the thought of effectively rendering my high fish diet useless is off-putting to say the least!
You can test the your omegas - have you done that?
Could be good to do a before and after
This is the test I use. Heard that it is better than normal blood testing labs because it looks at what’s in the cell membrane and hence gives you an average over time that is more stable/reliable (kind of like HbA1c vs just one blood glucose reading). Learned that it is what Peter Attia’s team uses after looking at different options.