A bit off topic here (but since you brought it up) I have always been puzzled why human reproductive age has such a huge gap between males and females, whereas in all (or at least most) animals I know of there is little or no difference at all? Would be interesting to see if any scientists ever tried to explain this. Reason i bring it up is because somewhere somehow (in my brain) I think that what works for men, may not work for women (for the most part) when it comes to longevity.
The U-shape observational studies have been superseded by trials like JUPITER which showed a big reduction (-20% from 1.25 to 1.0) in all cause mortality in the rosuvastatin group compared to placebo. Do not trust observational studies until Mendellian randomization proves causation!
1 Like
Fertility rates drop off for males too after the age of 40. Maintaining good sperm quality requires exercise and supplementation.
I thought the JUPITER trial was looking at the impact of rosuvastatin on men with median 108 mg/dL ldl-c. So quite a bit higher. Was there sub- analysis showing benefit below 50/60 mg/dl?
Hi, what are you targeting for apoB and hba1c?
1 Like
I like this, and i hadn’t read it.
I’ll go through it now
What you said has nothing to do with what I was saying. There was a 93 year old man that had a baby with his 32 year old wife a while back, and I think good old Al Pacino at 83 had a baby also.
1 Like
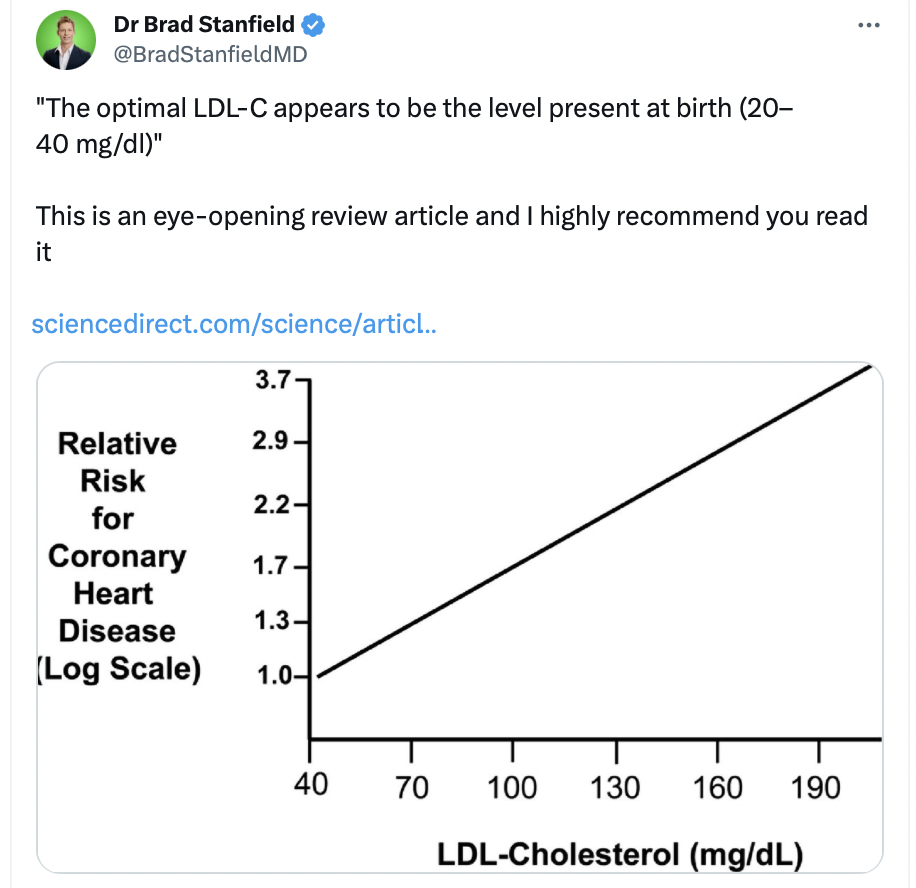
If LDL-C can be kept very low from birth, atherosclerosis will not occur.
“initiating lipid-lowering therapy after a person has already been exposed to a cumulative burden of 6250 mg-years of LDL by age 50 years means that person has very likely already developed a large atherosclerotic plaque burden … lowering LDL after this cumulative exposure to LDL should reduce the risk of cardiovascular events, but this person will remain at relatively high “residual” risk of experiencing an acute cardiovascular event because one of the underlying plaques can still disrupt to cause an acute coronary syndrome
Humans were never meant to harbor the low-density lipoprotein cholesterol (LDL-C) levels that are now commonplace. In one series of 147 full-term neonates, the average LDL-C was 20 ± 10 mg/dL [59] Despite the extraordinary rate of development and need for myelination, even neonates need very little LDL-C
a ‘normal’ non-atherogenic LDL-C level is 20–40 mg/dl.
Based on the log-linear relationship of LDL-C to the hazard ratio for an acute ASCVD event, the LDL-C level where no excess risk occurs is approximately 38 mg/dL or 1 mmol/L
2 Likes
I’ve just spotted some issues. This doesn’t look at the impact of statins, and is for secondary prevention only.
“nonstatin LDL-C–lowering therapy added to background statin therapy were included in the meta-analysis (Table 1). All 3 were secondary prevention trials that enrolled patients with known atherosclerotic cardiovascular disease.”
I like Peter Attia’s analogy that if you leave it until you’ve acvd, then you need to slam on the brakes. That’s what seems to be happening here.
Of the three rcts it references I’m familiar with two look at the third now
It is citing this study:
Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170 000 participants in 26 randomised trials
https://www.thelancet.com/action/showPdf?pii=S0140-6736(10)61350-5
1 Like
Is it possible to buy this drug from chemical synthesis?
https://www.nejm.org/doi/full/10.1056/nejmoa1706444
Anacetrapib, CETP inhibitor (-18% apoB, +36% apoA1)
2 Likes
This seems much nicer, but still not phase 3 trials completed yet:
https://www.reddit.com/r/PeterAttia/comments/140iakd/thoughts_on_obicetrapib/
1 Like
I have been taking rapamycin for 2 years. The only time I saw rapamycin affected blood sugar and cholesterol was at high doses. i.e. over an effective dose, taking GFJ into account was at doses that exceeded 20 mg/wk. There is no discernable effect on blood sugar or cholesterol at the dose I am taking, 4mg/wk. All of my lipid measures are good and towards the good end of the spectrum. Even when I was taking high doses the effect wasn’t large, though it did concern me at the time. Of course, I am one, and the results may vary.
4 Likes
From the paper you reference, still another of many supporting lower is better.
“Meaning Further lowering of LDL-C beyond the lowest current targets is associated with further reduced cardiovascular risk with no offsetting safety risks.”
I am not going to argue the benefits of statins, I am a believer in low to moderate doses. If you can’t get the results you want with low does statins, then try adding something like Pantethine, if that doesn’t work then add ezetimibe.
Currently, I am taking all three, atorvastatin 40mg, Pantethine 600mg, and ezetimibe 10mg.
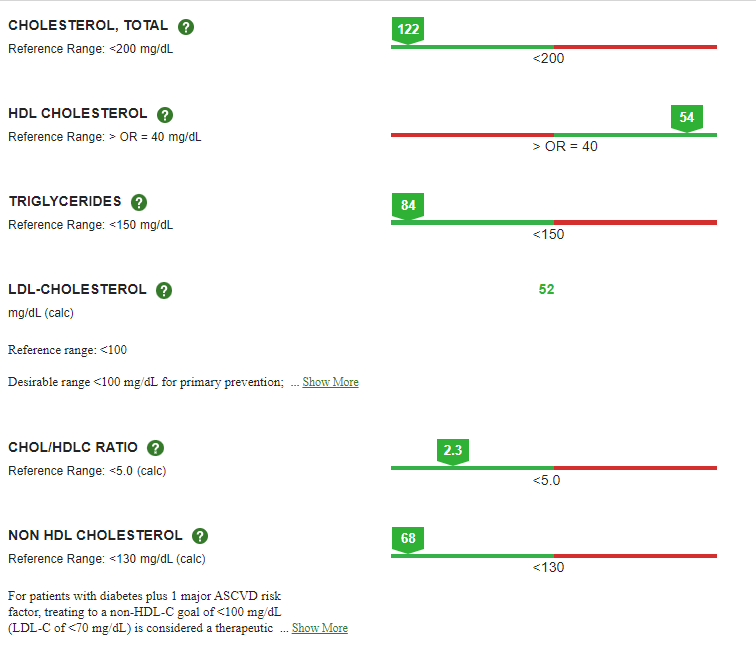
My latest results from taking the triple combo along with 4mg/wk of rapamycin with GFJ on 11/21/23.
This is the best result I have seen for some time. Also, I am on a low to moderate carbohydrate diet.
8 Likes
I’m taking reasonable steps to get below: apoB / 60 and HbA1c/ 5.5. If I fail, I will try harder but I’m steady for now.
My apoB is 48 (down from 74 12 mos & 64 6 mos ago)
My HbA1c is 5.5 (down from 5.8). I’d like to be lower but I’m focusing on sleep and stress improvement for further reduction.
ApoB: 10mg rosuvastatin every other day, 10mg ezetimibe 5 days/ wk, vit b5 500mg 5 days / week
HbA1c: metformin 500 mg 4 d/w, berberine 500mg 5 d/w, no added sugar in diet.
4 Likes
Is there a reason to do higher every other day vs lower every day?
1 Like
Longevity past reproductive age is not favored by evolution : the only reason humans could have evolved to live this long past female menopause is to have at least one sex capable of reproducing in old age. In fact, it also means all of us must have enough number of male ancestors that reproduced at an old age, to favor the genes that happened to favor longevity.
The only other land mammal where females live well past menopause are Asian Elephants. Technically other land mammals are said not to experience menopause, since females die of old age while still fertile, but most mammals have a gradual drop in female fertility with age, so the difference between strict menopause and very low female fertility past a certain age, as with African Elephants, is not that different in terms of evolution of longevity : in both cases longevity can only evolve if males remain fertile in old age.
1 Like
LDL-C is used as an approximation of ASCVD risk and as such it might be totally misinterpreted on individual basis. It is good to test atherogenic particles or composition of your LDL-C. For example my triglycerides and apoB are low and apoA1 are high in spite of my HDL-C being normal and my LDL-C rather high.
1 Like
An old off patent and cheap Bezafibrate might do just that. It is not a strong LDL-C lowering drug it might even elevate LDL-C if your TGs are rather high, that is why I imagine is not really popular among LDL-C lowering craze but it will affect your metabolic pathways, lowering TG, blood sugar and lowering atherogenic lipoproteins (apoB) and boosting non atherogenic lipoproteins (apoA1).