All cause mortality doesn’t only matter even if it’s important. It probably is there, just it wasn’t a long enough study duration. Or enough participants. Heart attacks lower quality of life and healthspan, which is why you can’t dismiss a study just because it couldn’t measure ACM benefit. But like I said it is often because of practical reasons you cant find a difference. It costs a lot to run long studies and/or with many participants.
That said it was brought up in the article I linked earlier that focusing on all cause mortality would bypass this adjudication process debate. You only measure amount of deaths in both arms and no rogue doctors can start making their own conclusions unblinded who died by what.
I saw that follow up study with ACM benefit but I didn’t understand why they didn’t have a p-value so I didn’t bring it up. Do you know why? And why we can be certain about the result?
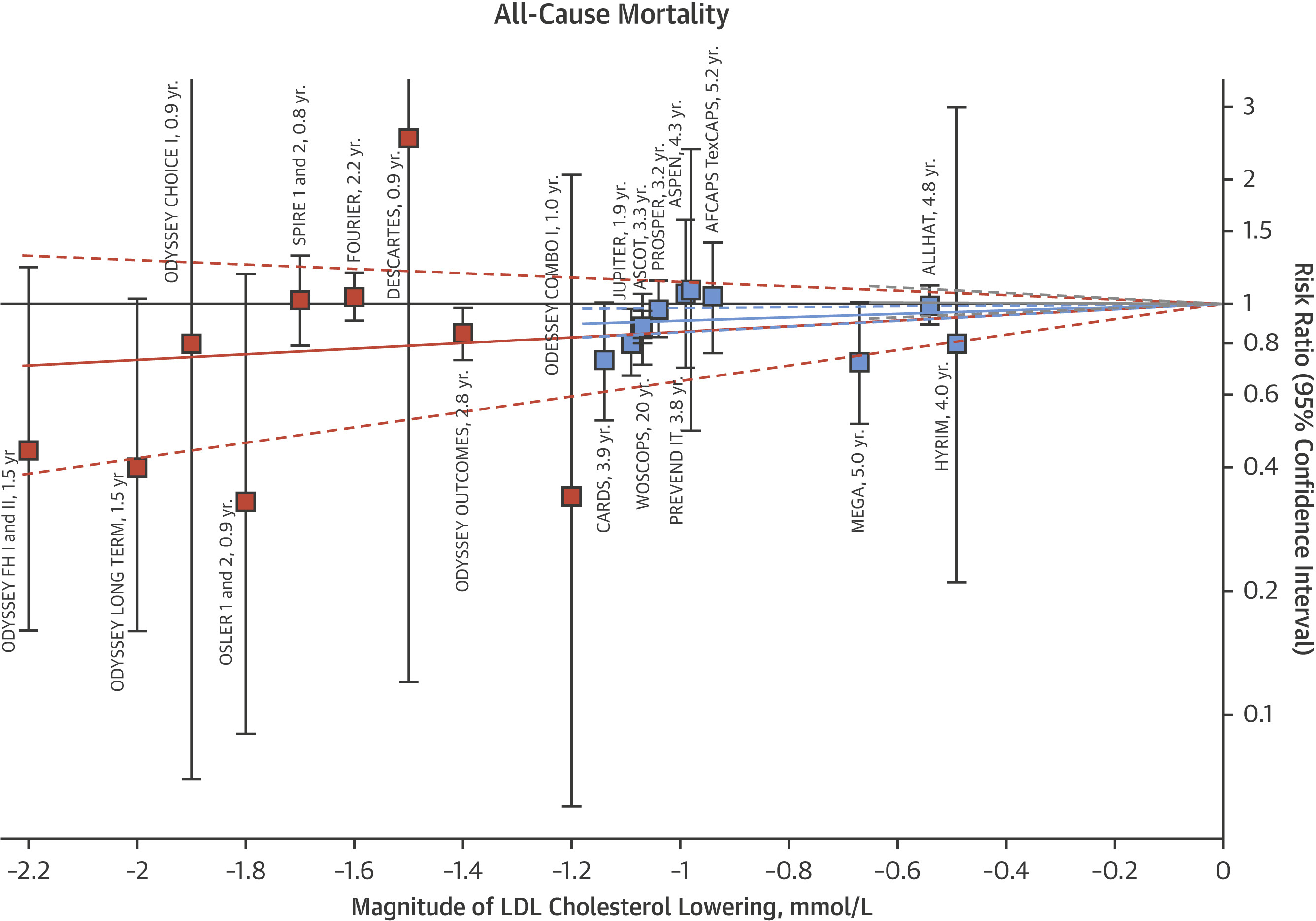
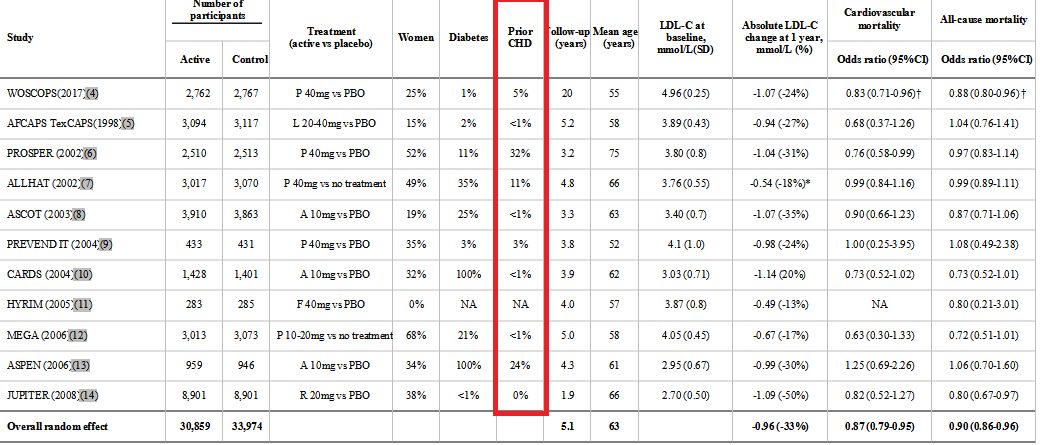
Meta analysis of 11 randomized controlled trials of over 65,000 people show no total mortality benefit for statin usage in primary prevention even in those with intermediate to high risk, except for those with known CVD.
I see no need for the person with an elevated LDL from rapamycin, free of underlying CVD, to take statins to prevent a primary cardiovascular event. My position hasn’t changed.
You cannot say it had no total mortality benefit if it wasn’t statistically significant.
You cannot say anything about a result if it was not statistically significant.
You do realize that significant means “statistical significance”, not “significant” as it’s commonly used?
“show no total mortality benefit” does not mean there wasn’t a mortality benefit.
Absence of evidence does not mean evidence of absence.
In the absence of preexisting cardiovascular disease, statins have no benefit in primary prevention to lower all cause mortality rates. This appears to be true even in the presence of other risk factors.
It is, however, quite good for secondary prevention.
Okay, interesting discussion.
I’ve now looked at all the trials.
All were about primary prevention. And in 2 studies of 11 were there people included with pre-existing disease, but not only (PROSPER and ASPEN). 9 of 11 trials were done with absence of preexisting cardiovascular disease.
Statins lower all cause mortality in primary prevention. Even without preexisting cardiovascular disease.
The weight of the evidence in favor of statins is so high in my opinion that it does not even merit further discussions at this time.
I see no harm in taking them, in fact, quite the opposite. It is unlikely that any long-term, double-blind RCT is going to take place anytime soon. Until that happens and it proves statins are not beneficial, I will happily keep on taking my daily dose of atorvastatin.
The ACM benefit is based on the amount of lipid reduction, for every 0.5 mmol/L LDL reduction a 5% lower ACM.
So it is precisely because of the lipid reduction.
Also remember these are short term trials. The MR and genetic studies show a very large decrease in ASCVD related events because of compounding benefits.
I think you missed the point: “I see no harm in taking them, in fact, quite the opposite.”
Plus, my doctor whom I respect, prescribed them, I didn’t ask for them.
I’m sure your cardiologist is very competent. Merely pointing out absolute risk reduction for purposes of discussion. Not attempting to diagnose or offer treatment advice.
Indeed. Statins do behave as HDAC inhibitors which serves to increase histones acetylation and expression of p21 in human cancer cells. Could be useful in that regard as a cancer fighter, but of course unrelated to lipids.
That’s an interesting point. If they only inhibit HDAC2, however, then I would think their effect on the availability of Acetyl-CoA is at least relevant. The level inhibition in the tens of micromolar is not out of line with many other HDAC inhibitors although the big question is the bioavailability of any one HDAC inhibitor.