I am not your doctor and I haven’t even seen you. Please don’t ask me whether you should go on a statin or not.
I’m certainly not going to be providing anything beyond general information and my nonexpert interpretation of the literature that should never be relied upon to make any sort of treatment decisions.
As mentioned, consider requesting a referral for a lipidologist.
I will mention there isn’t any human data to guide healthy individuals for long-term statin use (ie risk of tendinopathy), nor is HDL really a resolved issue. There is such a gross oversimplification on the immunological function of lipoproteins overall. AFAIK, Attia probably hasn’t mentioned it much at all. I don’t think he’s ever gone over statins, MMP, cartilage, and collagen. Or immunology much.
There is some evidence to even suggest some subtypes of HDL are atherogenic. We really don’t know as much as Attia claims.
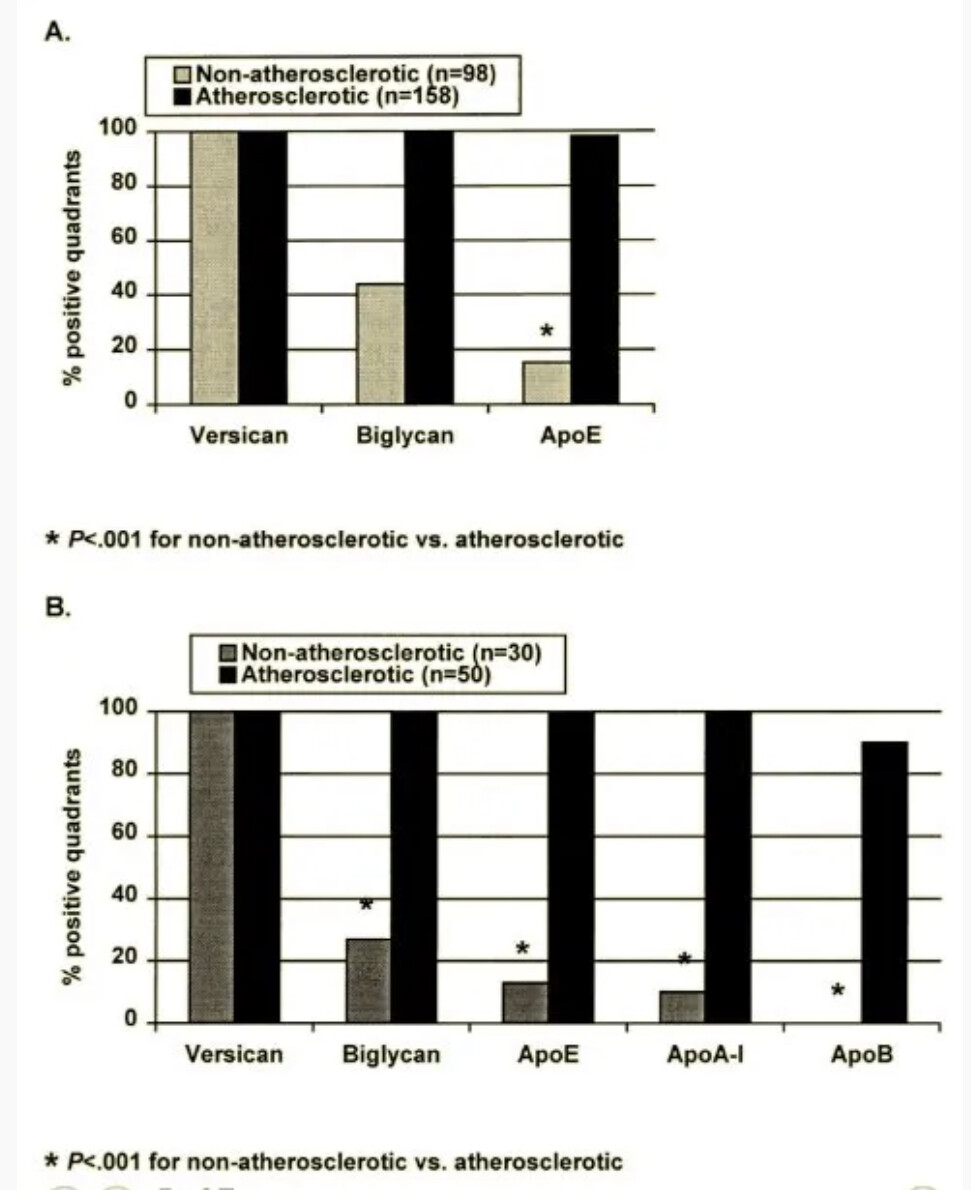
We can see here biglycan which is a proteoglycan that attracts apoB and apoE is in 100% of lesions - but apoE is present in almost 100% of lesions, apoA1 in 100%, and apoB, the supposed initiator, according to Attia, is only present in 90%. If you understand the basics of lipidology and assume Attia’s non-expert hypothesis was flawless, it should be 100% apoB - not 90%.
Now this does not mean anyone should stop a statin if they are indicated for one by their doctor or that apoB is irrelevant. I mentioned the weekly dosing with increased “hepatoselectivity” as an option to reduce risk of myopathy (or potential cognitive risks by avoiding specific statins that may significantly cross BBB) in those where it is indicated by their doctor to talk with their doctor about the benefits vs risks in statin switching - particularly those with risk enhancing factors for atherosclerosis.
It just means the mechanism isn’t as clear as purported and there’s a lot of real gaps. It’s easy to sell a vastly simplified story - “do something” in healthy people and pay me 6 figures per patient as VIP medicine, which has documented risks of its own. If there isn’t a big risk we are reducing - why trade one potential small benefit for several potential risks? There are other options that can be tried first. And even then Attia seems to have been off statins himself - I wonder why since he doesn’t appear to have explained it despite his “faith” in statins. Now if there was better evidence in the context I’m looking for or I’m indicated for it - I’d seriously consider taking a statin. I’m not claiming statins are super harmful drugs either - they’re relatively “safe” overall assuming perfect conditions and usage.
Seems to me that many people can potentially lower LDL from say 100-130 to 70-90 with say 12-15g 100% psyllium husk from food (especially if you have low soluble fiber intake), 5 grams of 100% cocoa bits from food, and/or “perfect” lifestyle factors alone - if you’re aiming for some target. If you’re not discordant - there probably isn’t significant potential benefit in absolute risk reduction from a target of 70-90 through daily combined statins/ezetimibe to say a target 55 in “healthy” people (55 may be a more reasonable target in certain high risk patients with history) with no risk factors. When Attia claims statins are so-called “compound interest” as an investment, that doesn’t take into account other systemic risks. If his position turns out to be true - why not take the route of “compound interest” with the lowest potential risks?