Hi,a little update for those who follow the story:
I have given up rapamycin completely and have modified my diet to minimize saturated fat (literally followed the boring guidelines). Not even religiously, just the general direction - less fatty meat, less dairy, more fish and lean meats.
In 4 months:
ApoB went from 113 to 73
Total Cholesterol 209 to 167
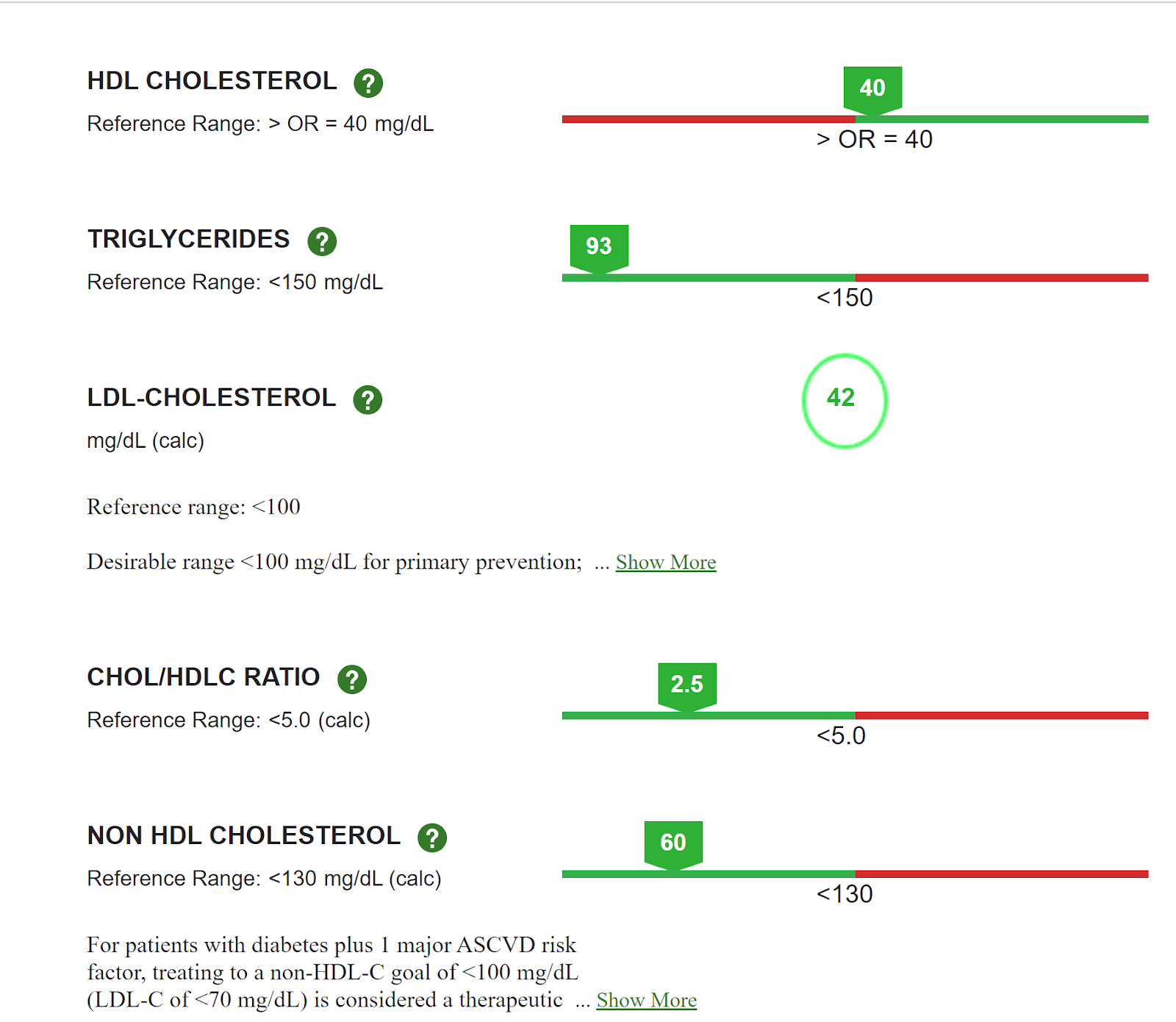
LDL Cholesterol from 133 to 89
Triglycerides from 63 to 58
Not sure how much of it can be attibuted to quitting rapa vs change in diet but I am willing to go back to low dose rapa and see what happens
Triglycerides were great pre- and post-change. So diet quality was probably quite good both before and after.
We can argue till the cows come home about whether the lower LDL, etc. are actually meaningful improvements for you. We need to be cautious about focusing on surrogate markers of health.
The data says your risk of heart disease is lower with these lipids. It is not so clear your expected longevity is meaningfully longer with these lipids. Your actual health history is relevant here, along with your risk factors for heart disease.
My guess is that the trade is strongly negative - off rapamycin but improved lipid panel → statistically lower expected longevity. But that assessment is based on some guesses about rapamycin’s benefit that are unproven. So obviously I may be wrong. (Although if I am, most of us taking Rapa are similarly wrong.)
Despite the fear that rapamycin raises cholesterol and glucose levels, I found that yes, it does have an effect, but I found it very easy to correct for it. In the case of cholesterol, I just added pantethine for cholesterol control and Linagliptin (5mg) for glucose control.
Before taking rapamycin my meds included metformin, 500 mg/day, and atorvastatin 40 mg/daily tablet. As I have previously posted: I am currently taking rapamycin 4mg/weekly with GFJ. My cholesterol levels are all in the low normal range and my HbA1c is 5.6%, which isn’t bad for my age.
Bottom line: Whatever effect rapamycin has on your cholesterol and/or glucose levels it is easy to bring them back to your previous levels by making lifestyle adjustments and/or adding supplements.
Apo B is casual, so would not see that as a surrogate marker.
In biology nothing is crystal clear, but the evidence is mounting in the direction that higher Apo B => lower life- and healthspan:
Mendelian randomization reveals apolipoprotein B shortens healthspan and possibly increases risk for Alzheimer’s disease
And
A trans-omic Mendelian randomization study of parental lifespan uncovers novel aging biology and therapeutic candidates for chronic diseases
And
Effects of apolipoprotein B on lifespan and risks of major diseases including type 2 diabetes: a mendelian randomisation analysis using outcomes in first-degree relatives
Apo B is a surrogate marker for health. You won’t find a death certificates in the US that list the cause of death as “high ApoB”.
ApoB is not a health outcome per se, which is why it is a surrogate marker for health. That doesn’t mean it is not important but one does want to treat the patient holistically, not the lab values.
Anyway, as reported, “ApoB went from 113 to 73”
How much additional life expectancy does that correspond to in your opinion? I guess you might have a number or a range since you disagree with the statement that “It is not so clear your expected longevity is meaningfully longer”.
So how much longer is it? Or, maybe we agree it is not so clear?
And then we have the question of: is this expected improvement from reduced ApoB greater than the expected reduction from stopping Rapamycin? My guess is that tradeoff is negative but that is just a guess.
We don’t even know if the doses used by humans have any effect on lifespan. What we do know is that ASCVD is the leading cause of death in humans (not in mice) so treating apoB (and other risk factors) is of utmost importance. The choice is not binary though as you can take multiple medications at the same time to get the best of both worlds.
A drug that improves lifespan in mice, rapamycin, is not expected to offset this effect from this data. That’s why it’s going to be important. It will attenuate any lifespan improving effect either way, so you are worse off with higher lipids and a bottleneck on your longevity.
Given current information, if I had to choose between a statin and rapamycin I would choose statins in a heartbeat because I don’t know if the rapamycin dose and frequency I can afford would help prolong my life but I do know that statins will lengthen my lifespan.
Luckily I do not have to choose between either and can take both because the world is not binary.
But the lipid numbers on a statin will likely be even lower if you drop Rapamycin, correct?
So while the world is not binary, one still is going to have to consider this question of whether somewhat elevated lipids + Rapamycin is better for longevity than somewhat lower lipids + no Rapa.
Which is why I think one needs to look at the entire context of the patient: age, gender, various risk factors, untreated lipids, treated levels, etc. And admit we are uncertain, but taking our best guess.
Probably, but anything below 70mg/dL is probably sufficient for now, given I’m addressing multiple risk factors at the same time. Once new lipid therapies become generic I’ll start treating more aggressively.
whether somewhat elevated lipids + Rapamycin is better for longevity than somewhat lower lipids + no Rapa.
It depends on what you consider “elevated”. If it’s above 70-80mg or so, you should probably drop rapamycin or use a higher statin dose.
And admit we are uncertain, but taking our best guess.
Ideally we would aggressively treat lipids to levels below 40mg/dL alongside taking high dose rapamycin every couple days in accordance with the ITP protocol. Obviously that approach is prohibitively expensive and likely to negatively affect your immune system so that’s not viable.
Currently, I am working to maintain the same levels but increase HDL a little. I have recently added benzoic acid. I expect my next blood test to have even lower levels and hopefully raise HDL levels.
I was responding to this - the bold part - how someone likely would interpret you holistic point (not semantics about different definitions):
Apo B is casual for the largest killer in the western world, CVD (and most disability yielding disease in stroke and heart attacks), so what I mean is that you (and the person you were talking to and others that will read your strong statement) absolutely should focus on their Apo B if they want to healspan and longevity optimize.
How much additional life expectancy does that correspond to in your opinion? I guess you might have a number or a range since you disagree with the statement that “It is not so clear your expected longevity is meaningfully longer”.
So how much longer is it? Or, maybe we agree it is not so clear?
The exact quantification or “number” is not clear. (Thought the papers that I and @A_User pointed you to and dozens of other comments we’ve made on the topic that you can search here on the forum can give some idea).
At the same time, it likely is a materially large effect seems increasingly clear based on the trial and Mendelian Randomization data. That should probably be enough to optimize for it in a Medicne 3.0 / longevity optimization approach.
And then we have the question of: is this expected improvement from reduced ApoB greater than the expected reduction from stopping Rapamycin? My guess is that tradeoff is negative but that is just a guess.
What is your thought on that question?
My main view of that question is that you actually don’t have to choose - you can figure out a holistic approach to Apo B optimization even if pulled up a bit by rapa, might eg include adding the cheap and seemingly safe ezetimibe, re calibrating statin use, optimizing diet, etc.