Website: https://strongermemory.org

This report provides a clinical and critical distillation of the StrongerMemory program, a non-pharmacological cognitive intervention developed by Rob Liebreich (CEO, Goodwin Living). The summary integrates the provided transcript with evidence from George Mason University and Tohoku University research.
I. Executive Summary
The core thesis of the StrongerMemory program is that daily, low-anxiety engagement in three specific neuro-stimulatory tasks—reading aloud, handwriting, and rapid simple math—can stabilize or improve cognitive function in individuals experiencing Mild Cognitive Impairment (MCI) or subjective cognitive decline. Mechanistically, these tasks are designed to maximize blood flow and activation in the prefrontal cortex and hippocampus, regions primary to memory encoding and retrieval that often show reduced activation in aging populations Kawashima et al., 2012.
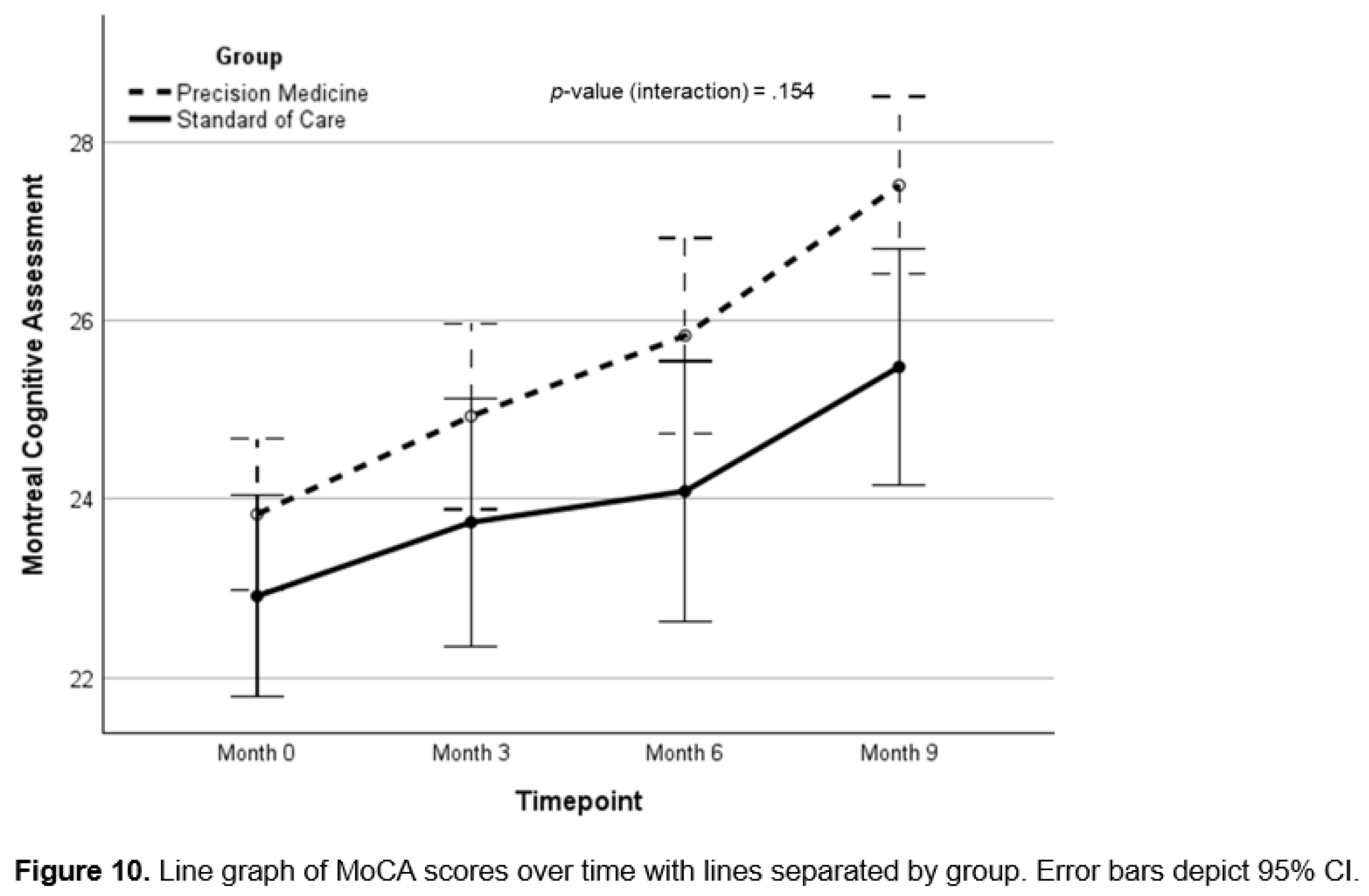
The program transitions cognitive health from a passive, pharmaceutical-dependent model to an active, habit-based “brain exercise” regimen. Recent quasi-experimental data from George Mason University indicates significant statistical improvements in cognitive scoring for participants following a 12-week protocol Ihara et al., 2025. Critically, the intervention demonstrates a “transfer effect,” where training in simple arithmetic and literacy improves non-targeted executive functions and processing speeds.
Furthermore, Phase II research suggests that while solitary practice is effective, the integration of social engagement(group reading/sessions) creates a synergistic effect, enhancing emotional well-being and longitudinal durability of the cognitive gains Kang et al., 2025. Field data from a three-year CMS-funded pilot involving 91 nursing homes reported that 76% of participants experienced perceived or actual cognitive stabilization, challenging the standard narrative of inevitable decline in institutional settings.
II. Insight Bullets
- Prefrontal Cortex Target: The protocol specifically targets the prefrontal cortex (directly behind the forehead), which governs memory retrieval and executive function.
- Reading Aloud vs. Silent: fMRI data confirms that reading aloud engages language factories and auditory circuits, providing significantly higher brain activation than silent reading.
- Handwriting vs. Digital: Handwriting requires complex fine motor integration and spatial processing that typing lacks, aiding in more robust memory encoding.
- The “Speed Over Accuracy” Rule: In the numeracy component, the objective is rapid processing (working memory) rather than mathematical complexity; high-anxiety math creates counterproductive stress chemicals.
- 23-Minute Threshold: Data suggests an average of 23 minutes of daily engagement is the “minimum effective dose” for measurable cognitive benefit.
- Longitudinal Durability: Research indicates that cognitive gains can persist for up to six months even after the 12-week intensive period ends, though daily habituation is recommended.
- Transfer Effects: Stimulation of the prefrontal cortex through these tasks “spills over” into unrelated tasks, such as general intelligence and creativity.
- Social Synergy: Group participation (social engagement) yields higher cognitive and emotional outcomes than solitary practice.
- Institutional Efficacy: 76% of nursing home residents in a CMS pilot showed improvement, suggesting the brain remains plastic even in late-stage care settings.
- Language Versatility: The program is currently validated in English, Korean, and Japanese, suggesting the biological response is language-agnostic.
- Early Intervention Window: The program is most effective for Mild Cognitive Impairment (MCI) and “subjective decline” rather than late-stage Alzheimer’s.
- Intergenerational Benefits: Use of the program in “reading circles” with youth addresses both cognitive decline and senior isolation (loneliness).
- Non-Pharmacological Safety: Zero side effects are reported, making it a high-safety adjunct to standard care.
- Cost-Free Scalability: The program is offered for free via the StrongerMemory foundation to bypass the financial barriers of memory care.
III. Actionable Protocol
High Confidence Tier (Level A/B Evidence)
- Reading Aloud: Engage in 10–15 minutes of vocalized reading daily. This can include books, newspapers, or religious texts. The key is the auditory-vocal loop Kawashima et al., 2005.
- Handwriting Practice: Spend 5–10 minutes writing by hand. Transcription of text or journaling is sufficient; the mechanical movement is the primary driver of the benefit.
- Simple Numeracy: Perform 5–10 minutes of rapid, simple math (e.g., single-digit addition). Focus on “speed of processing.” Do not use a calculator.
- Frequency: Minimum 4–5 days per week. The “Gold Standard” for maximum neuroplasticity is 7 days per week.
Experimental Tier (Level C Evidence)
- Social Integration: Perform the reading aloud or math components within a “reading circle” or group setting. Preliminary evidence suggests this increases adherence and emotional resilience Kang et al., 2025.
- Combination with Movement: Integrate physical exercise (e.g., walking) as a primer for the cognitive exercises to increase cerebral blood flow.
Red Flag Zone
- Replacement Fallacy: Do not use this program as a replacement for prescribed Alzheimer’s medications or clinical oversight. It is an adjunct.
- Complexity Trap: Avoid “hard” math or complex puzzles that cause frustration. If the task induces high stress, the cortisol response may negate the metabolic benefits to the prefrontal cortex.
- Digital Translation: Current evidence is specific to handwriting and vocal reading; digital brain games have not shown the same degree of “transfer effect” to real-world memory in all populations.