Source: https://x.com/DrSamuelBHume/status/2040369629986504844?s=20
7 Likes
Global study finds combined pollution and inequality can accelerate brain aging
An international study published across 34 countries shows that the biological age of the brain can be accelerated or delayed by environmental risk (air pollution, public housing conditions) and protective factors (socioeconomic equality, access to health care). The stronger effects arise from interactions among environmental, social, and political conditions. The paper is published in Nature Medicine .
Using data from 18,701 individuals across 34 countries, the study shows that the exposome (the cumulative set of environmental, social, and sociopolitical exposures that individuals experience throughout life) operates in a syndemic manner—when two or more health problems occur together and interact in a way that makes each other worse—with multiple co-occurring exposures having very large effects, shaping brain aging across both healthy individuals and those with neurodegenerative conditions.
The researchers quantified 73 different environmental factors measured at country level indicators spanning air pollution, climate variability, green space, water quality, socioeconomic inequality, and multiple indicators of political and democratic contexts. When modeled jointly, these factors explained up to 15 times more variance in brain aging than any single exposure alone.
This finding highlights a key shift: environmental influences on brain health are cumulative and nonlinear, with interactions across domains amplifying their biological impact.
Paywalled Paper: The exposome of brain aging across 34 countries (Nature)
1 Like
From what’sapp…
Website:
We just announced BrainYears — a clinically validated brain age clock (EEG and ERP based with MRI-grade accuracy in collaboration with the Buck Institute).
This gives clinics a new category:
→ Brain aging diagnostics
→ Measurable treatment validation
→ New revenue across testing + therapyWe’re selectively onboarding the first 10 clinics.
Watch the video for details and if you know anyone interested please have them message me directly. Thanks.
Maybe it’s been posted before…
Based on their results, the researchers hypothesise that they may have found a solution to the chicken-or-egg scenario between amyloid-beta peptides and tau tangles – although we should bear in mind that their experiments were with mixtures of purified proteins. Understanding how proteins behave inside cells is far more complicated.
If amyloid-beta peptides displace tau from its usual binding sites, as these protein studies suggest, then this might explain how tau can knot itself in tangles and microtubules become destablized, disrupting core functions of neurons and ultimately leading to cell death…
The brain’s cleaning system can be boosted to rid Alzheimer’s proteins
A duo of drugs that boosts our glymphatic system, which clears waste from our brain, also improves the removal of proteins associated with the onset of Alzheimer’s disease
Drugs that boost our brain’s waste-disposal system so it can better remove proteins associated with Alzheimer’s disease have been identified for the first time. The combination of a therapy that is commonly used as a sedative with a medicine that prevents dangerously low blood pressure seems to safely and effectively remove proteins linked to the disease, which could delay its onset by seven years.
“This is a significant step forward,” says Shiju Gu at Harvard University, who wasn’t involved in the research. “It could benefit people with neurodegenerative disease, but even for healthy people, maybe you could use it to maximise the function of the brain.”
Researchers have previously found that dexmedetomidine, a drug commonly used as a sedative during medical procedures, boosts these brain waves in mice. It also improved the brain’s ability to clear waste fluid and slowed cognitive decline in mouse models of Alzheimer’s disease.
To explore dexmedetomidine’s effects in people, Paul Dagum at pharmaceutical company Applied Cognition in Redwood City, California, and his colleagues recruited 19 adults – aged 60, on average – who were deprived of sleep for one night in a lab. The morning after, the participants – who had no chronic medical conditions or brain-specific issues – provided blood samples to act as baseline measurements.
They were then given 4 hours while they received an infusion of dexmedetomidine. They also took a drug called midodrine, which treats low blood pressure, a common side effect of dexmedetomidine. When they woke, the participants provided another blood sample.
This revealed that taking dexmedetomidine and midodrine, which the company collectively calls ACX-02, cleared two amyloid and tau proteins that are particularly prone to misfolding and forming clumps more effectively than the placebo/saline intervention.
The team estimates that if ACX-02’s effect were sustained over several years, it could delay the onset or worsening of Alzheimer’s disease by about seven years, based on levels of misfolded amyloid that are typically seen in people who go on to develop the condition, says Dagum. “That would be a significant, meaningful effect for those at risk,” adds team member Jeff Iliff at the University of Washington in Seattle.
Full story: The brain’s cleaning system can be boosted to rid Alzheimer’s proteins (New Scientist)
Related Research Paper:
Pharmacological enhancement of glymphatic function in humans increases the clearance of Alzheimer’s disease-related proteins
4 Likes
Dexmedetomidine: Dexmedetomidine - Wikipedia
Dexmedetomidine, sold under the brand name Precedex among others, is a medication used for sedation.[4] Veterinarians use dexmedetomidine for similar purposes in treating cats, dogs, and horses.[10][11] It is also used in humans to treat acute agitation associated with schizophrenia or bipolar disorder.[5] It is administered as an intravenous solution or as a buccal or sublingual film.[1]
There are no known contraindication to the use of dexmedetomidine. It has a biphasic effect on blood pressure with lower readings at lower drug concentrations and higher readings at higher concentrations.[32] Common side effects include: hypotension, hypertension, with slight decreases in heart rate, arrhythmias, and hypoxia.[33][34] Toxic doses may cause first-degree or second-degree atrioventricular block. These adverse events usually occur briefly after administering a loading dose of the drug. Thus, adverse effects may be reduced by omitting a loading dose.[34]
Midodrine: Midodrine - Wikipedia
Midodrine, sold under the brand name Proamatine among others, is an antihypotensive medication used to treat orthostatic hypotension (low blood pressure when standing) and urinary incontinence.[1] It is taken by mouth.[1]
Side effects of midodrine include hypertension (high blood pressure), paresthesia, itching (pruritus), goose bumps, chills, urinary urgency, urinary retention, and urinary frequency.[1] Midodrine is a prodrug of its active metabolite desglymidodrine.[1] This metabolite acts as a selective agonist of the α1-adrenergic receptor.[1] This in turn results in vasoconstriction and increased blood pressure.[1]
1 Like
Brain injured? Maybe avoid EPA.
Eicosapentaenoic acid reprograms cerebrovascular metabolism and impairs repair after brain injury, with relevance to chronic traumatic encephalopathy
https://www.cell.com/cell-reports/fulltext/S2211-1247(26)00213-5
1 Like
That’s a spooky graph.
What about Somatic (non-heritable) E2/2 gene editing? Is anyone working on that for prevention?
Alzheimer’s disease is one of the hardest unsolved problems in medicine, and one of the most devastating. It kills millions of people, places a huge burden on families, and still defies much of what medicine can do today. At the OpenAI Foundation, we want to change that by using advanced AI to accelerate the science of preventing and treating the disease. As a first step, we are working to finalise more than $100 million in grants this month, across six research institutions, to support and accelerate Alzheimer’s research—generating new data, helping design new drugs, and expanding possible paths to treatment…
Announced today:
3 Likes
Of course, there is always a gotcha.
"For individuals with the APOE E2/E2 genotype, lifestyle recommendations focus on managing specific metabolic profiles that differ from the more common E3 and E4 variants. While E2/E2 is often considered “protective” against Alzheimer’s, it carries a unique risk for Type III hyperlipoproteinemia, which can lead to high triglycerides and premature heart disease. "
1 Like
If money and researcher time were used for developing a non-heritable homozygous E2 gene therapy I presume any downsides and pleiotropic benefits would be thoroughly researched and how it would be modified.
The simplest answer to AD prevention seems to be this by looking at that graph.
I remember someone posted their lipid levels with E2 allele and they had like a natural apoB of 50 mg/dl, so it might even prevent ASCVD (now that I think about it, if it lowers apoB that much that might be a reason why AD decreases).
Not all E2/E2 appear to have that side effect:
However, only a minority of apo ε2 homozygotes become hyperlipidemic, often due to metabolic conditions that either increase lipoprotein production or decrease remnant clearance
Data from the UK Biobank indicate that apo E2 homozygosity is present in 0.2–1.3% of individuals, depending on genetic ancestry (23), and less than 20% of those with the apo E2/E2 phenotype develop overt hyperlipidemia (22), despite having demonstrable β-VLDL in the plasma, characteristic of dysbetalipoproteinemia.
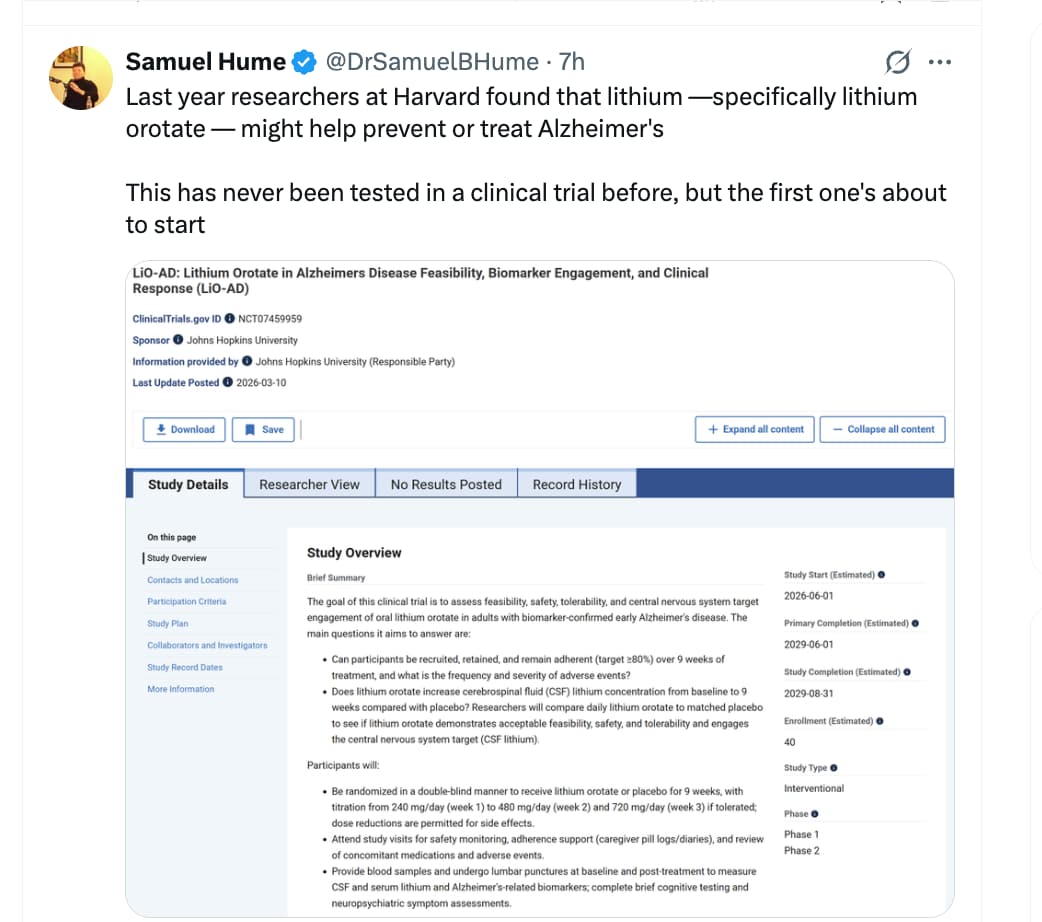
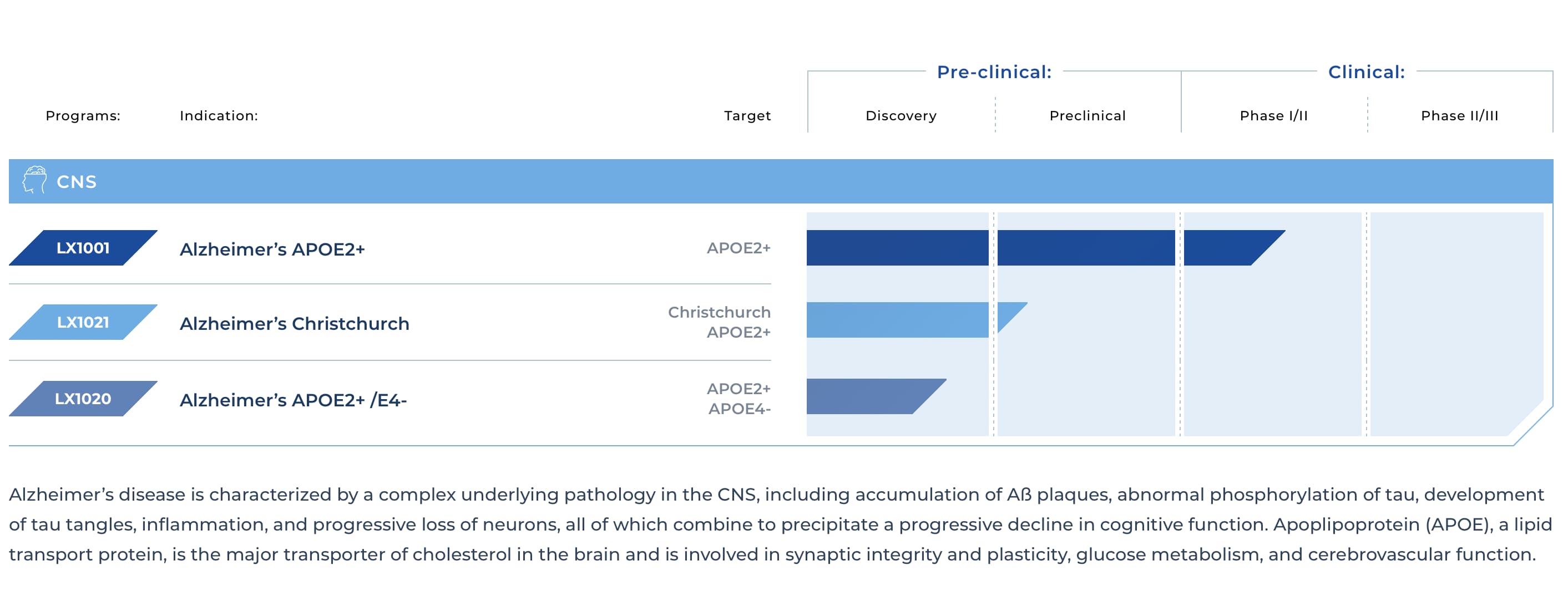
There’s a company called Lexeo working on gene editing to get people to express apoe e2 in their central nervous system. Alzheimer’s - Lexeo Therapeutics
Phase 1/2 trial results: https://alz-journals.onlinelibrary.wiley.com/doi/10.1002/alz70859_101538
Result
Fifteen participants were dosed: 50% MCI, 14% mild and 36% moderate dementia, at baseline. Twelve months of data are available for C1-C3 and 6 months for C4. Treatment with LX1001 was generally safe and well-tolerated. No events of amyloid related imaging abnormalities were observed. Post-treatment, APOE2 was expressed in CSF in all participants in a dose dependent manner. Interim results showed stabilization in CSF Aβ42/40 and amyloid PET. There was a decrease in CSF t-tau, p-tau, and Tau PET. Full data results including 12-month data for C4 will be presented during the meeting.
3 Likes
Are we sure the pessimistic graph of Alzheimer’s disease rates is for the average population?
The note to the graph in Nature states, “ Kaplan–Meier curves were generated from Alzheimer’s dementia cases and cognitively unimpaired non-AD controls in the neuropathologically confirmed group. Y -axis represents the percentage of persons with each APOE genotype in the neuropathologically confirmed group who remained free from Alzheimer’s dementia. X -axis denotes age at death for controls and age at onset of cases, while replacing with age at death when age at onset was unavailable.”
It seems like the population in the graph wasn’t an average population, but I would appreciate help from others to assess this.
Also, this graph does not appear to be in line with other Alzheimer’s rate studies based on APOE status. Can anyone provide some clarity here?
2 Likes
This Gemini summary suggests prevalence at 100 is about 50% to 60%
2 Likes
Inflammaging and the Aging Brain: How Adiposity and Micronutrient Deficits Drive Cognitive Decline
Aging is characterized by creeping, low-grade systemic inflammation—often termed inflammaging—that chronically degrades cognitive reserve. A newly published pilot study provides a granular exploration into the nexus of dietary constituents, lifestyle behaviors, and progressive cognitive decline. The investigators demonstrated that older adults presenting with a high body mass index (BMI) exhibited significantly elevated plasma concentrations of pro-inflammatory cytokines, most notably tumor necrosis factor-alpha (TNF-α). Concurrently, altered interleukin-10 (IL-10) profiles were observed in these individuals, pointing to a severe disruption in basal anti-inflammatory regulation. Similar pro-inflammatory cascades, characterized by surges in TNF-α, interleukin-6 (IL-6), and IL-10, were prevalent among participants with low physical activity metrics.
When evaluating dietary habits against European Food Safety Authority (EFSA) dietary reference values, the findings introduced compelling anomalies. Participants ingesting excessive quantities of carbohydrates and polyunsaturated fatty acids (PUFAs) demonstrated demonstrably poorer cognitive performance across specific memory and learning domains. Conversely, individuals consuming higher amounts of saturated and monounsaturated fatty acids displayed superior cognitive function. This unexpected result challenges entrenched nutritional dogma regarding saturated fats and underscores an ongoing scholarly debate regarding the necessity of specific lipid structures for preserving neural integrity during advanced aging. Furthermore, inadequate overall caloric intake—frequently championed as a proxy for lifespan-extending caloric restriction pathways—was associated with significantly higher error rates in memory tests. This indicates a critical threshold where energetic deficits become neurologically deleterious rather than protective.
Specific micronutrient deficiencies also proved highly toxic to both inflammatory homeostasis and cognitive health. Dietary inadequacies in vitamin B12 and magnesium were strongly correlated with elevated systemic inflammatory markers. Meanwhile, insufficient intake of essential trace minerals like manganese and copper was directly linked to degraded cognitive outcomes. Ultimately, while preliminary, this pilot data strongly reinforces the premise that optimal brain aging, neuroprotection, and overall healthspan extension demand strict precision in both metabolic maintenance and micronutrient sufficiency.
Open Access Paper: The impact of dietary constituents on inflammation and cognitive function in healthy older Irish adults: A pilot study
Context This research was conducted by the University College Cork in Ireland. It was published in the journal Nutrition and Health.
Impact Evaluation The impact score of this journal is 1.4, evaluated against a typical high-end range of 0–15+ for top nutrition science, therefore this is a Low impact journal.
1 Like
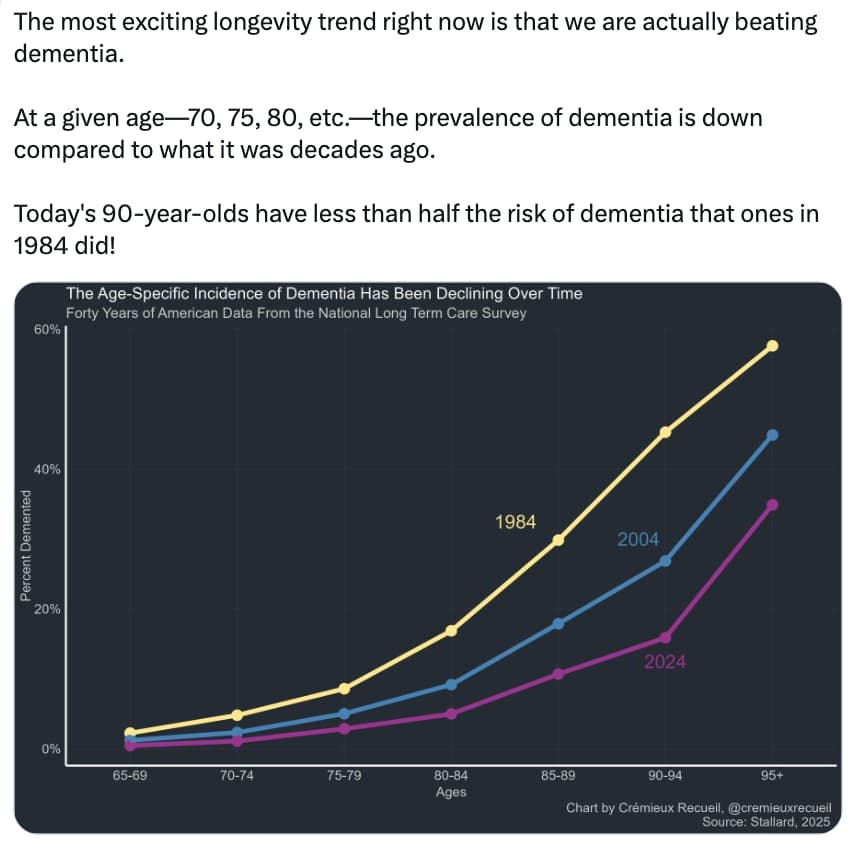
Yes, that’s because half of the dementia risk factors are preventable, and we’ve been better at addressing high cholesterol, hypertension, diabetes, etc.
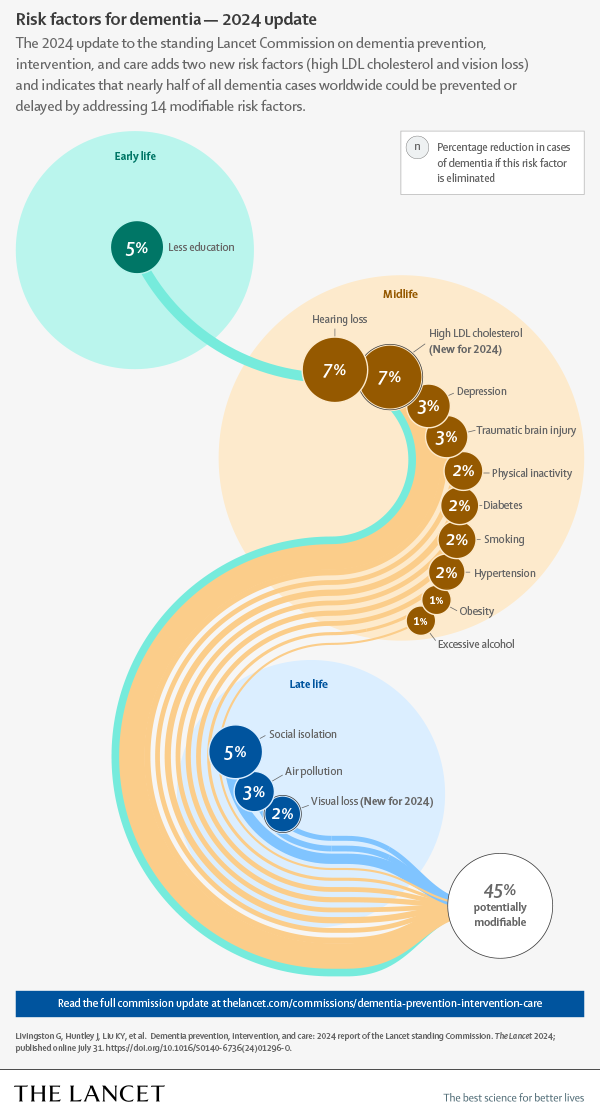
For the remaining half, though, we have no clue, so we’ll reach a ceiling…
4 Likes
News article about that paper: Scientists Uncover Potential Brain Risks of Popular Fish Oil Supplements
Albayram stressed that the findings should not be taken as a blanket warning against fish oil use. “I am not saying fish oil is good or bad in some universal way,” he said. “What our data highlight is that biology is context-dependent. We need to understand how these supplements behave in the body over time, rather than assuming the same effect applies to everyone.”
He hopes the research encourages closer examination of both the benefits and limits of omega-3 supplements. The study focused on a specific condition, repeated mild traumatic brain injury, and used CTE tissue to provide supporting evidence rather than to prove direct cause.
“As with any study, there are important boundaries,” Albayram said. “In the human CTE tissue, we can observe patterns, but we cannot prove what drove them. We also cannot capture every variable that shapes omega-3 handling in real life, including overall diet, health status, and lifestyle.”
The next step, according to the team, is to better understand how EPA is absorbed, transported, and distributed in the body, especially through fatty acid transport systems. “This paper is a starting point,” Albayram said, “but it is an important one. It opens a new conversation about precision nutrition in neuroscience, and it gives the field a framework to ask better, more testable questions.”
Highlights from the paper itself:
- EPA exposure after TBI unmasks a latent cerebrovascular vulnerability
- EPA reprograms endothelial metabolism, impairing vascular repair and remodeling
- EPA-driven neurovascular instability promotes tauopathy and cognitive decline
- Findings reveal metabolic context as key to omega-3 effects in brain injury
7 Likes
Symptoms of early dementia reversed by bespoke treatment plans
People with cognitive decline or early-stage dementia saw their symptoms improve when given bespoke treatment plans that targeted their personal nutritional deficiencies, ongoing infections and environmental exposures
A personalised programme that combines targeted medical interventions with lifestyle changes seems to improve memory and functioning among people with mild cognitive decline or the early stages of dementia. This involves assessing someone for factors that could be affecting their cognition – such as mould exposure, infections or hormonal deficiencies – and creating a bespoke plan to target them.
Dementia is an umbrella term for several conditions that affect memory, thinking and the ability to perform daily activities. It has no cure, with treatment generally focusing on relieving symptoms. But for Alzheimer’s disease – which makes up about 60 to 70 per cent of dementia cases – some drugs, like lecanemab, can clear the sticky protein plaques that form in the brain and are thought to contribute to the condition.
However, many have argued that these don’t improve people’s symptoms in a meaningful way. This may be due to the complexity of Alzheimer’s and other forms of dementia, which, evidence increasingly suggests, involve age-related changes in the brain as well as genetic, health and lifestyle factors. “[Patients] didn’t get well because we weren’t treating what was causing it in the first place,” says Kat Toups at Bay Area Wellness, a private practice in Walnut Creek, California.
Now, she and her colleagues have investigated the potential of bespoke treatment plans. “The approach is: let’s find all the things that are hurting the brain [and] get rid of those,” says Toup. “Then let’s put back in whatever the brain and the whole body is needing as far as nutrients and hormones, and then let’s do things for neuroplasticity to help regain your brain.”
The team recruited 73 people – aged 65, on average – with mild cognitive impairment or early-stage dementia. “Some of them met [the] criteria for Alzheimer’s and others for MCI [mild cognitive impairment],” says Toups.
They all underwent testing to identify potential contributors to their symptoms. Alongside blood tests to look for biomarkers of Alzheimer’s, the researchers assessed their levels of inflammation and checked whether they had any underlying infections or hormonal, nutritional or microbial-related deficiencies. Using this information, the researchers created personalised treatment plans for 50 of the participants, such as addressing nutritional deficiencies via supplements.
They were also told to adopt a plant-rich diet, do aerobic and strength training six days a week, and complete daily cognitive training via games that targeted their memory, attention and visual-processing speed. This group was also given tips to optimise sleep and manage stress.
The remaining 23 participants continued with their usual treatment and lifestyle habits.
After nine months, those in the personalised group saw their overall cognitive score – assessed by CNS Vital Signs, a standard computer-based cognitive test – improve by 13.7 points, compared with a decline of 4.5 points in the standard-care group. Improvements were also seen across specific domains within the test, including memory (up by 10.6 points versus a decline of 2.7), executive function (up by 9.8 versus down by 2.2) and processing speed (up by 6.9 versus down by 1). “Over 90 per cent of the patients in the precision-medicine approach had statistically significant improvements,” says Toups.
Full story: Symptoms of early dementia reversed by bespoke treatment plans (New Scientist)
2 Likes
I do wonder what the corresponding known 0% was in 1984 though. And what the corresponding % will be in 5 years time.
I would argue that we do have “clues” as to the remaining half. This from Gemini suggests we’ll be at 65% modifiable in 10 years. With AGI ot could be much higher
“Factors Expanding the Prevention Percentage
The “preventable” percentage is rising because researchers are identifying more environmental and biological triggers that we can control:
2017 (35%): Identified 9 factors including hearing loss, hypertension, and obesity.
2020 (40%): Added 3 factors: air pollution, excessive alcohol, and head injury.
2024 (45%): Added high LDL cholesterol and vision loss.
Future Projections (Up to 65%): Emerging frameworks now include “structural” factors like poverty, wealth shocks, income inequality, and HIV infection rates.”
Is there any evidence of a ceiling? The trendline suggests that there’s no slowing of our improving ability to avoid/delay dementia. And all other things being equal AI should accelerate prevention