If you are not actually improving blood sugar handling then you should not expect an improvement in parkinsons. This, of course, raises two questions
a) would the dysregulation of blood sugar (temporary) from Rapamycin argue against the use of Rapamycin for parkinsons. (or argue for very intermittent usage).
b) would activity to improve glycemic control in non diabetics improve Parkinsons.
Antoine and I had a useful discussion with the people at the event.
High-dose metformin is associated with a higher rate of PD. So, glycemic control is insufficient and should not come at the expense of mitochondrial health. That’s why SGLT2i seem interesting in PD: glycemic control + mTOR inhibition (see Figure 1 here). But they’re mild.
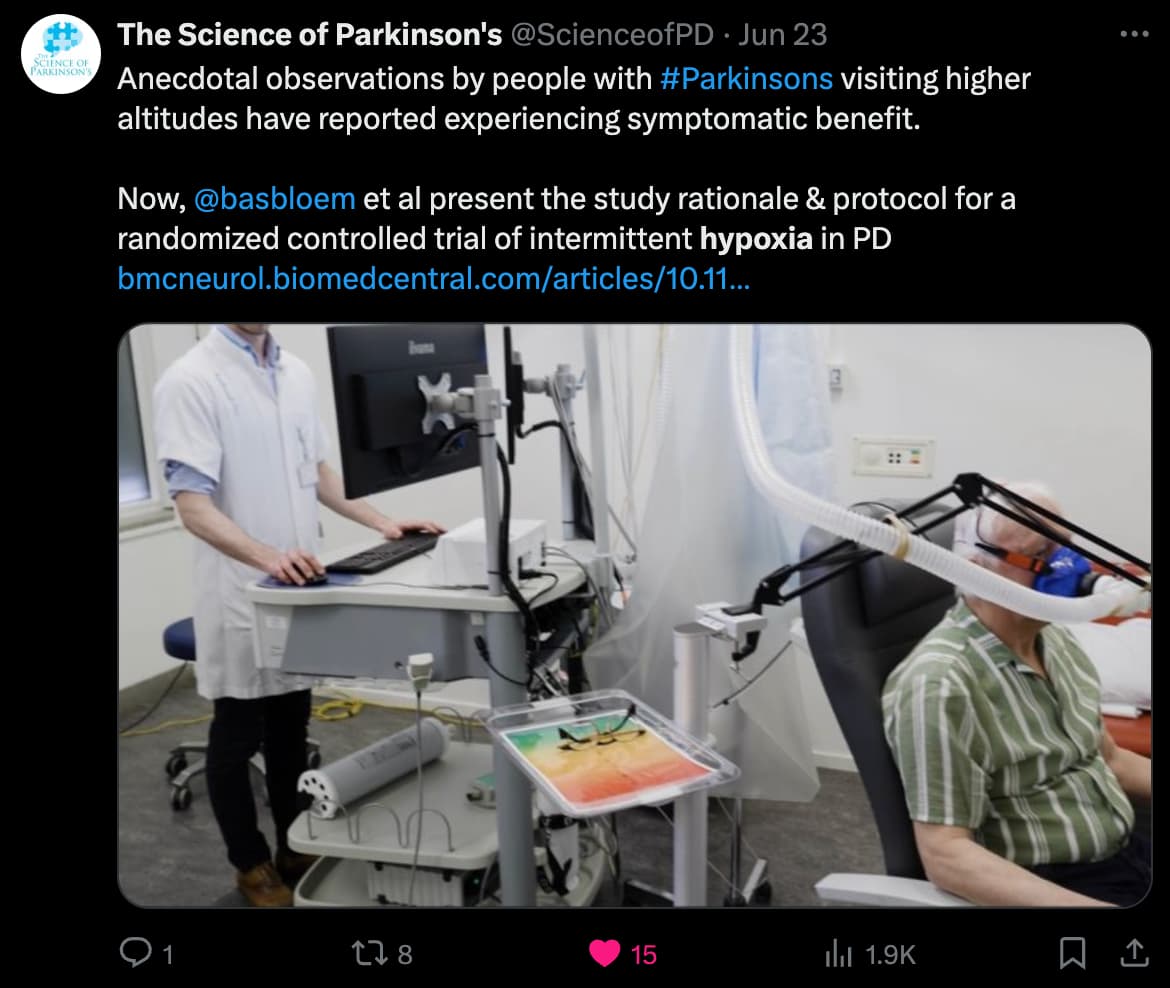
However, what’s interesting is that many Parkinson’s patients report that their symptoms improve (or totally stop) at high altitudes (including in an airplane). So, in a HYPObaric environment. There’s an ongoing trial for that.
Interventions will be conducted three times a week, for four weeks in total.
five times five minutes hypoxia interspersed with five minutes of normoxia, totaling 45 min
The thing is that it is the reduction in partial pressure that does the job of starting HIF 1 alpha. That can be done at a normobaric pressure, but starting with a higher concentration of Oxygen. I do this using an Oxygen concentrator.
Independent of its function as a precursor for DA synthesis, we demonstrated that l-DOPA can mediate both, a neurotoxic and a neuroprotective activity. Interestingly, the precise kind of action depends directly on the oxygen tension. Under normoxic oxygen levels, auto-oxidation of l-DOPA and linked ROS production prevails, while under hypoxic conditions l-DOPA auto-oxidation is heavily reduced.
So overall our data suggest an oxygen-dependent dual effect of l-DOPA: Under normoxic conditions l-DOPA auto-oxidation produces cytotoxic ROS, whereas under hypoxia and during shorter treatment duration l-DOPA is more stable and the ROS scavenging capacity prevails. Moreover, we observed that neuronal cell lines were much more vulnerable than other human cell types to l-DOPA-mediated ROS.
Oxygen partial pressure will be an issue, but specifcially in getting the HIF 1 alpha nuclear factor initiated it is the change in pressure that makes an issue.
You wrote “At this point I will assume that switching on HIF from time to time is “a good thing”. Therefore, we need to know how to switch on HIF.” So I’m putting these here without context:
More and more we’re finding the importance of the gut biome to the immune system. This latest information on gut biome and Parkinson’s might be of interest to some people.
The fix might be as simple as increasing certain vitamins and supplements like B2 and B7. On a similar vein, for decades ulcers were treated with surgeries that did not prevent the reoccurrence.
We realize that treating with antibiotics can cure certain ulcers. You don’t hear about ulcers the way you use to.
No relationship was observed between dairy consumption (HR 1.07, 95% CI 0.82–1.39), individual dairy products (milk: HR 0.95, 95% CI 0.73–1.23; yogurt: HR 1.03, 95% CI 0.82–1.29; cheese: HR 1.13, 95% CI 0.85–1.51), or vitamin D (HR 1.08, 95% CI 0.80–1.45) with PD risk. However, we observed a risk-increasing association with higher calcium intakes (HR 1.33, 95% CI 1.00-1.78, p for trend = 0.031), which was more pronounced in men (HR 1.50, 95% CI 1.00-2.25, p for trend = 0.044) and in ever smokers (HR 1.64, 95% CI 1.06–2.53, p for trend = 0.014). No compelling evidence was found for an association between dairy products or vitamin D intake and PD risk indicating a potentially limited relevance of dairy intake in PD risk than previously described. Our observations of a positive association between dietary calcium intake and PD risk in men and in ever smokers require further validation.
This suggests that vitamin D may not be related to the development of PD and that other mechanisms might therefore be responsible for the results in the aforementioned studies on serum vitamin D levels. One Mendelian randomization study explored the association between genetically decreased 25-hydroxyvitamin D concentrations with PD in individuals of European descent from 15 cohorts to investigate a potential causal relationship. The authors concluded that there is a lack of definite evidence supporting a role of vitamin D in PD.
On the other hand, men at risk of PD might prefer to avoid dairy products:
This suggests that vitamin D may not be related to the development of PD and that other mechanisms might therefore be responsible for the results in the aforementioned studies on serum vitamin D levels. One Mendelian randomization study explored the association between genetically decreased 25-hydroxyvitamin D concentrations with PD in individuals of European descent from 15 cohorts to investigate a potential causal relationship. The authors concluded that there is a lack of definite evidence supporting a role of vitamin D in PD.
I think the key role of Vitamin D is to maintain the bodies optional systems that only function when there is more food available. Hence the VDR enables optional genes. These may help with lot of things, but do not prevent diseases of aging.
I think it is clear that PD is a disease of aging as it occurs with age. I start then with the assumption that there is a problem with certain proteins being produced probably as different splices when power levels in the cells go down.
If it is a splicing issue (and there is evidence for this) that would explain a variation between people are different alleles will result in different splices at lower levels.
Hence although I think Vitamin D is someone to keep at a high serum level I don’t think it is an anti-aging vitamin per se.
I know identical twins, age 80. Both have severe arthritis.
One has been on methotrexate and its predecessors for 10-20 years and is mentally sharp. The other was diagnosed with fronto-temporal dementia 5 years ago.
Confounders: twin with dementia was much more sedentary, ate poorly, had untreated hyper-cholesterolemia, had a heart attack in late 40s, had children much later in life, was less social.
riboflavin orally (30 mg every 8 h) plus their usual symptomatic medications and all red meat was eliminated from their diet
All 19 patients who completed 6 months of treatment showed improved motor capacity during the first three months and most reached a plateau while 5/19 continued to improve in the 3- to 6-month interval. Their average motor capacity increased from 44 to 71% after 6 months, increasing significantly every month compared with their own pretreatment status (P < 0.001, Wilcoxon signed rank test). Discontinuation of riboflavin for several days did not impair motor capacity and yellowish urine was the only side effect observed.
After adjustment for potential dietary and non-dietary confounding factors, intake of folate, vitamin B12 and riboflavin was not associated with the risk of PD (P for trend = 0·87, 0·70 and 0·11, respectively).
At least one epidemiology study suggests that MTX (methotrexate) doesn’t increase risk for Parkinson (for RA patients although RA is correlated with higher risk for Parkinson).
Interestingly, chloroquine and hydroxychloroquine reduced risk by about 25% for Parkinson.
Perhaps it’s been brought up, but Klotho is mediated through Platelet Factor 4 in the brain and Dana Dubol has shown that PF4 is almost completely protective in PD neurons (not motor neurons). Unlike Klotho, PF4 is readily available for human use for 20+yrs.(used in a surgery setting). Human doses are already published; safety is excellent and I think Dubol was using 1 sq inj every 2-3 wks. I will dig up the paper, but if I had PD I would certainly consider PF4. Lots of different suppliers