We find an association in men who are taking Tz/Dz/Az and a lower hazard of DLB compared with similar men taking other medications. When combined with the literature of Tz/Dz/Az on Parkinson disease, our findings suggest that glycolysis-enhancing drugs may be broadly protective in neurodegenerative synucleinopathies. A future randomized trial is required to assess these associations for causality.
The UI researchers think that a specific side effect of the drugs targets a biological flaw shared by DLB and Parkinson’s disease, as well as other neurodegenerative diseases, raising the possibility that they may have broad potential for treating a wide range of neurodegenerative conditions.
For the new study, the UI researchers used a large database of patient information to identify more than 643,000 men with no history of DLB who were newly starting one of six drugs used to treat benign prostatic hyperplasia (enlarged prostate).
Three of the drugs, terazosin, doxazosin, and alfuzosin (Tz/Dz/Az), have an unexpected side effect; they can boost energy production in brain cells. Preclinical studies suggest that this ability may help slow or prevent neurodegenerative diseases like PD and DLB.
The other drugs, tamsulosin and two 5-alpha-reductase inhibitors (5ARIs) called finasteride and dutasteride, do not enhance energy production in the brain and therefore provide a good comparison to test the effect of the Tz/Dz/Az drugs.
In addition to BPH (benign prostatic hyperplasia), alpha-1 blockers like terazosin are also used in resistant hypertension (after ARB + DHP CCB + Thiazide-like at max dose failed to reach BP goals).
Could low-dose terazosin be interesting for neuroprotection in men with elevated BP @DrFraser?
Half of males above 50 suffer from BPH, so should they all take terazosin rather than finasteride?
The alpha blockers, like terazosin have a few side effects, and I wonder how much of this is dose dependent, as dosing is 1-10 mg. Postural hypotension, hypotension, tachycardia, somnolence, nervousness are among the common ones. If it was good at 1 mg … probably low rate of side effects … at 10 mg … might find a few with head injuries from passing out with standing.
The terazosin DDD for BPH is 5 mg, so we can assume it was the dose used by men in the above study. So 5 mg might already be neuroprotective. Can we go even lower? The trials are using 2 to 10 mg (as the target dose), so we’ll soon know. Also: what about low-dose but long-term accumulation? Could 1 mg per day for 10 years be as good as (if not better than) 10 mg per day for one year in terms of neuroprotection?
Role of Tau Protein in Neurodegenerative Diseases and Development of Its Targeted Drugs: A Literature Review ; PMC11206543.
Both theoretical about pathways involved and about possible therapeutical strategies for Alzheimer, Parkinson and other “tauopathies”. Summarizes in text numerous substances researched sofar or still in research and results sofar.
We additionally identified one FDA-approved drug associated with decelerated biological aging: the alpha-blocker doxazosin. We show that doxazosin extends healthspan and lifespan in C. elegans.
While no drug of the 500 + FDA approved drugs we assessed passed significance following a correction for multiple hypothesis testing (Benjamini and Hochberg), one compound—doxazosin—passed significance using a stringent unadjusted p-value cutoff (p < 0.01) (Figure 4E). Users of doxazosin were more likely to have negative deltaAges, representing a possible age-deceleration due to the drug, when compared to all others in the same demographic population.
As stated above, the association between doxazosin and decelerated age does not necessarily mean it causally benefits healthy aging. We therefore turned to C. elegans to test if doxazosin was causally geroprotective.
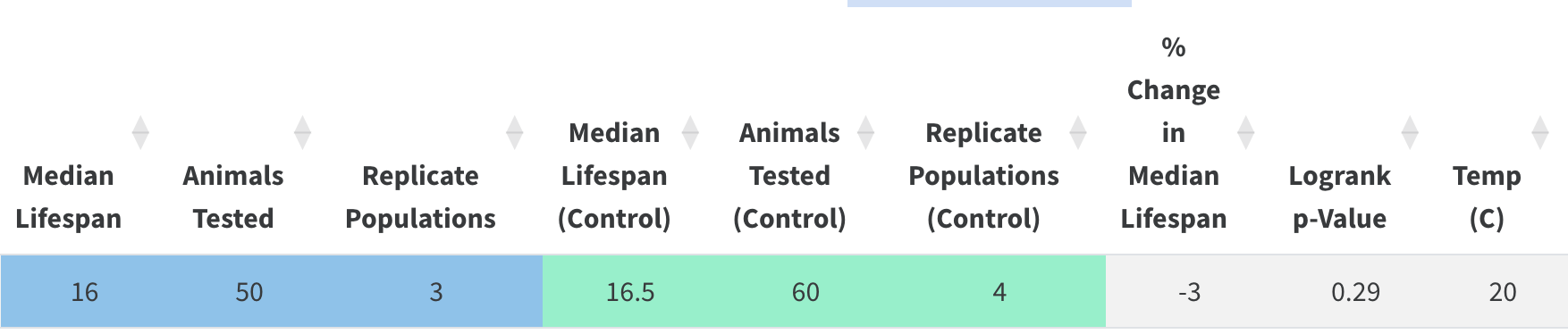
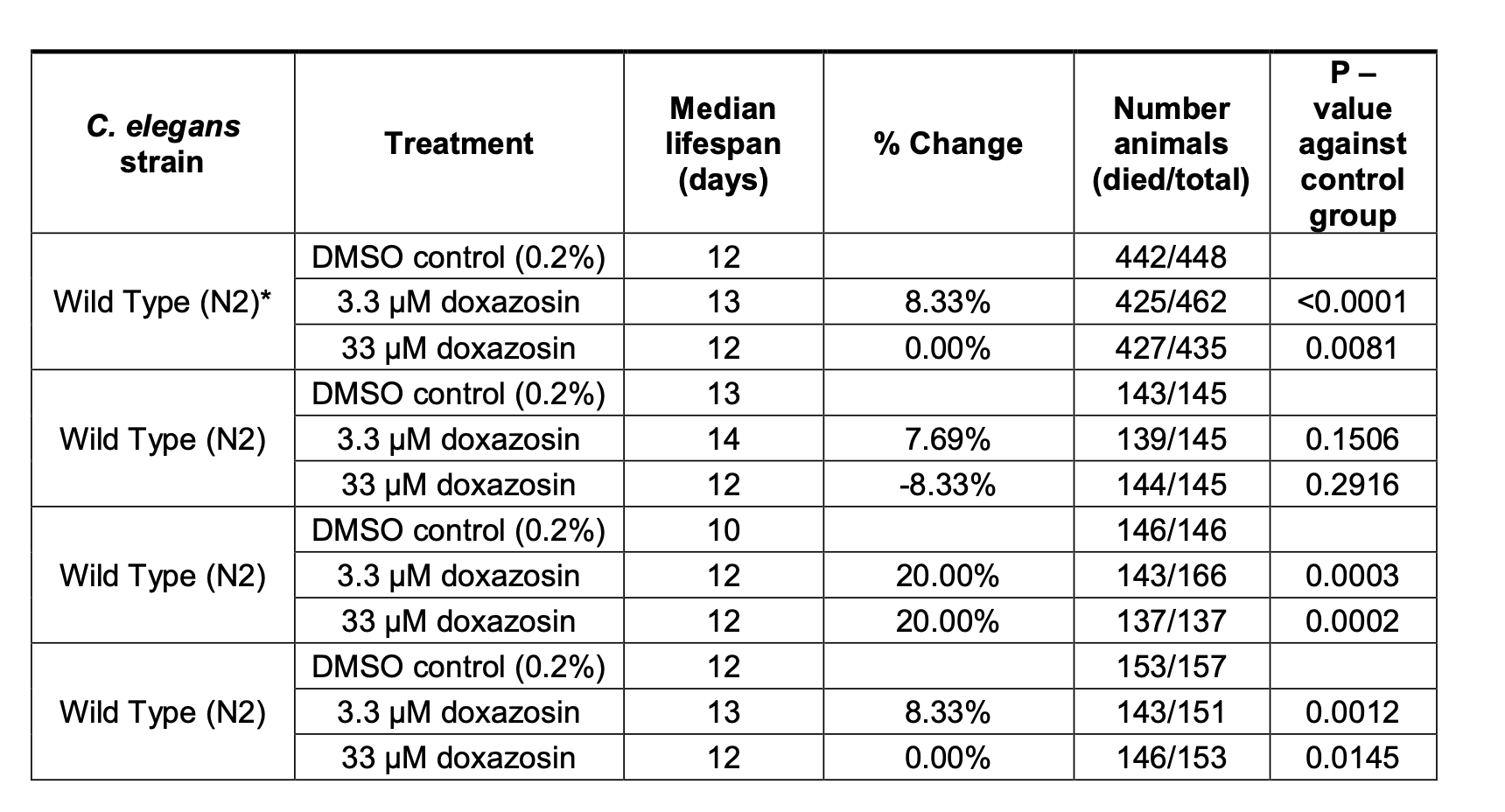
We then used a microfluidics platform totest lifespan and healthspan. Here we used multiple doses of doxazosin (3.3 and 33 μM) as previous observations show that microfluidics devices provide more direct drug contact than agar plates, and therefore a lower dose is needed (Hewitt et al., 2018). Indeed, we saw the greatest beneficial effects at 3.3 μM.
We confirmed that doxazosin extended worm lifespan (p < 0.0001) (Figure 4H; Supplementary Table 4) and simultaneously studied worm motility so as to measure healthspan via locomotion. With automated locomotion measurements, we calculated what percentage of worms remained highly active (defined as moving a distance greater than their body length in a 30 s window). Upon doxazosin treatment, we observed a higher percentage of highly active animals throughout life, particularly in the later ages tested, confirming their improved healthspan (Figure 4E; Supplementary Table 5). Altogether, we conclude that doxazosin extends both lifespan and healthspan in C. elegans.
The paper and its authors look good (although the journal is not great). So potentially lower doses are better for longevity (in worms at least…) @DrFraser!
I’ve just emailed Ora Biomedical to reproduce the above paper. Wait and see…
This study was based on a total of 678 433 BPH patients, out of which 287 080 patients belonged to the TZ/AZ/DZ cohort and 391 353 patients belonged to the tamsulosin cohort. The pooled incidence of PD was higher in tamsulosin users (1.28%, 95% CI: 1.04–1.55%) than in TZ/AZ/DZ drug users (1.11%, 95% CI: 0.83–1.42%). The risk of occurrence of PD was significantly lower in patients taking TZ/AZ/DZ than tamsulosin (n= 610,363, HR = 0.82, 95% CI = 0.71–0.94, P = 0.01; I2 = 87.4%).
(Note: A 3-month supply of doxazosin 1 mg costs 2 USD on IndiaMart…)
That doxazosin result looks like a pretty classic case of p-hunting. They tested something like 450 animals in each condition and found an 8% increase in lifespan. While statistically significant, I would be disinclined to believe it is biologically relevant. The survival curve presented and the data in the table are pretty unimpressive, although they worked very hard to show it (and get it published).
We can test it, but I bet the effect isn’t robust enough for us to statistically resolve it. We aim with our system to find large-effect size interventions (>25% increase).
Eighteen healthy men and women (60 – 85 years old) were stratified into two cohorts based on maximum TZ dosages (5 mg and 10 mg daily). Methods included plasma and cerebrospinal fluid TZ concentration measurements, whole blood ATP levels, 31Phosphorous magnetic resonance spectroscopy for brain ATP levels, 18F-FDG PET imaging for cerebral metabolic activity, and plasma metabolomics.
Our results indicated that a 5 mg/day dose of TZ significantly increased whole blood ATP levels and reduced global cerebral 18F-FDG PET uptake without significant side effects or orthostatic hypotension. These effects were consistent across sexes. Higher doses did not result in additional benefits and showed a potential biphasic dose-response.
Third, what is the dose-response relationship for TZ’s impact on energy metabolism in people? This point is relevant because TZ showed a biphasic effect on energy metabolism in mice, suggesting higher doses might counteract the potential energetic benefits.
This study provides insight into the relationship between the dose/concentration of TZ and its metabolic effects. For both ATP/Hb levels in whole blood and brain FDG uptake, a dose of 1 mg/day TZ did not significantly alter values, while 5 mg/day yielded significant differences and 10 mg/day did not generate further changes. These results are consistent with findings that the relationship between TZ concentration/dose and the activity of PGK1 as an isolated protein, in cells and in animals, is biphasic; low TZ concentrations increase activity and high concentrations inhibit PGK1. The biphasic response is an inherent property of the TZ:PGK1 interaction and we recently provided a molecular explanation for this unusual behavior.
Another signal for low-dose neuroprotective use of alpha blockers @DrFraser? (not too low though…)
As adssx mentioned an article of the same research group in the previous post this not be about Lewy body dementia because per wikipedia that starts most often at age around 50 with death within 4 years on average. So the study on TZ must be judged in its own right and may be of greater interest for may of us.
Alpha 1 blockers have been used for more than 30 years and they’re in the top 200 most prescribed drugs in the US. So if that’s 18 cases in history that’s very very very low. But good to know for someone with a personal or family history of priapism.
In several patients, priapism resolved following discontinuation of tamsulosin and recurred after its reintroduction. Both in the published and unpublished data, for majority of the cases, the time to onset of priapism was within few days following the first intake of tamsulosin.
So far, there are no studies that explored the dose–response relationship of tamsulosin and priapism. Besides, in all of the cases including both the retrieved and published ones, where dose of tamsulosin was reported, there was no issues of overdose except in one case. Thus, more information is required to conclude on this criterion.
Tamsulosin is more selective so it’s supposed to have fewer side effects and it’s way more commonly used (top 24 drug in the US, considering that it’s almost only used by men it’s huge): The Top 300 of 2021
So maybe the risk is higher for terazosin / doxazosin. But it’s hard to find data.
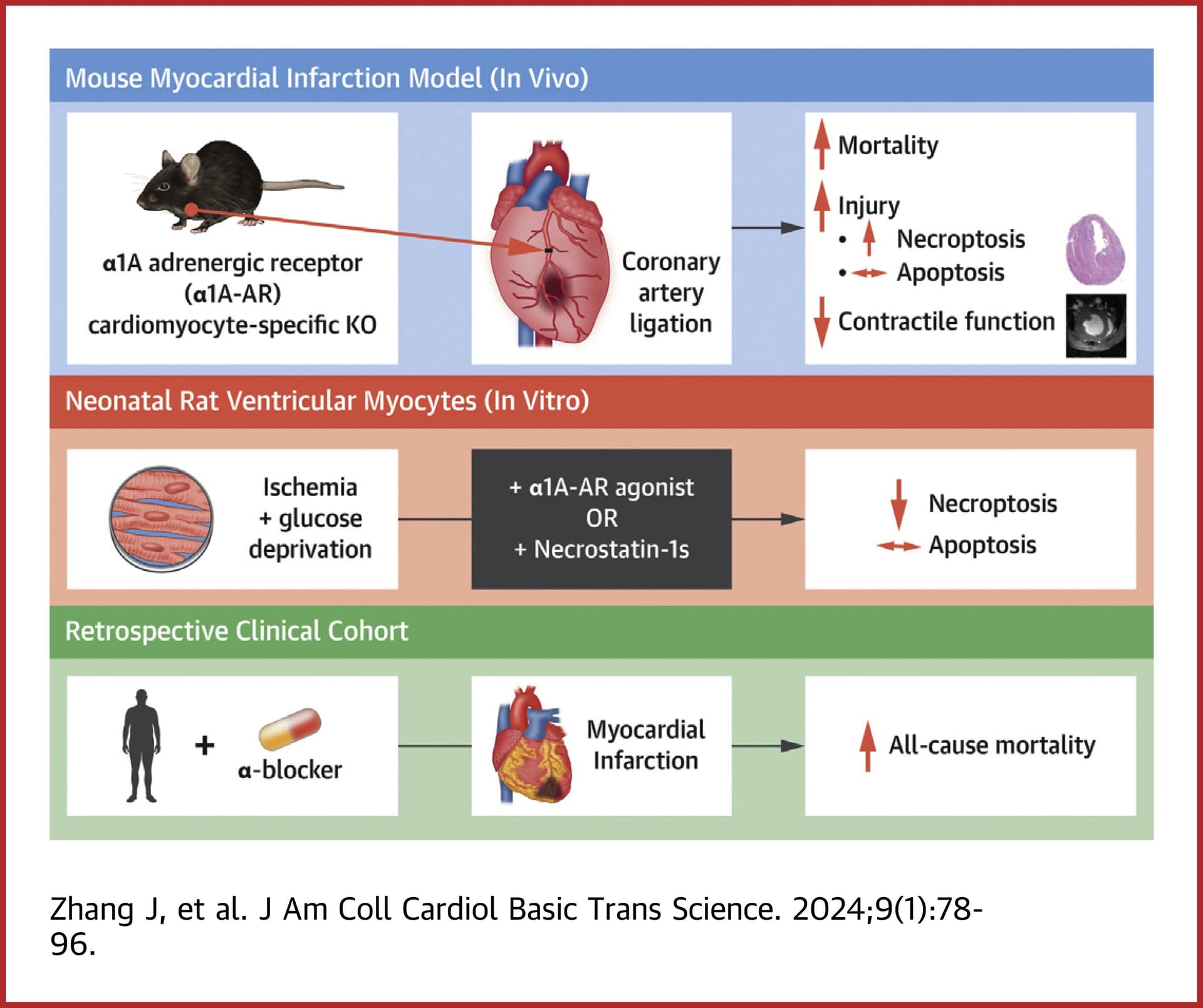
In our single-center clinical study, the use of α-blockers increased risk of mortality after MI, the first demonstration that these commonly used drugs may impact survival in high-risk patients.
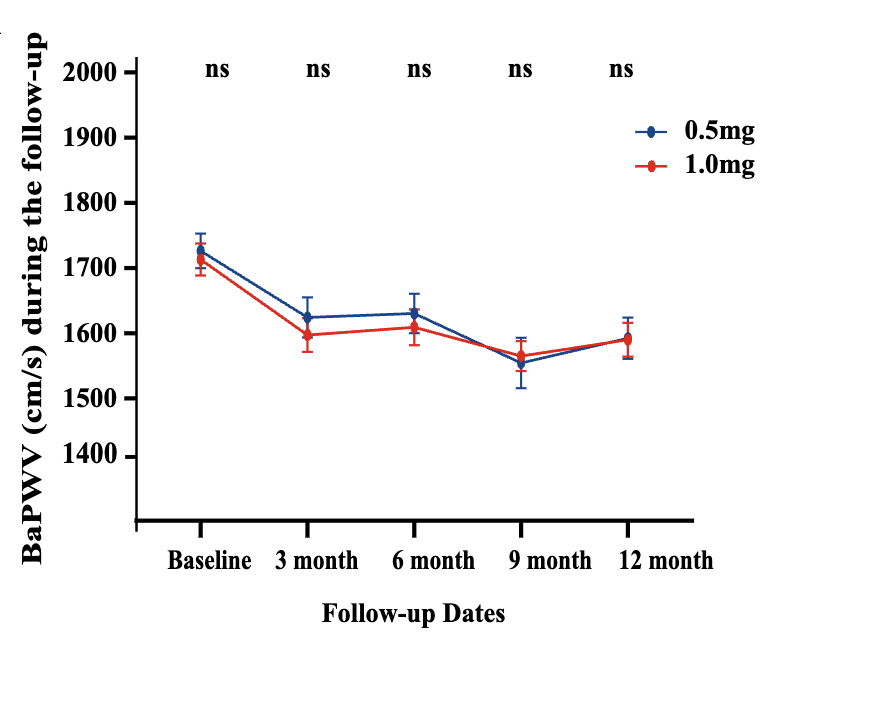
We enrolled patients aged over 40 with elevated arterial stiffness, defined as a brachial‐ankle pulse wave velocity (baPWV) ≥1400 cm/s, who were administered Terazosin (0.5 and 1.0 mg/day) from December 2020 to June 2023.
(1) Arterial stiffness significantly improved (at least a 5% reduction in baPWV) in 50.0% of patients at 3 months, 48.6% at 6 months, 59.3% at 9 months, and 54.4% at 12 months, respectively. (2) Those with higher baseline baPWV and hypertension exhibited a significantly reduced risk of non‐response. (3) Terazosin was associated with a reduction of baPWV at 1‐year follow‐up (linear regression: β = −165.16, p < 0.001). This pilot study offers valuable insights into the potential significance of Terazosin in improving arterial stiffness and paves the way for future randomised clinical trials in combating vascular ageing.
Terazosin, an α 1‐adrenergic receptor antagonist, has demonstrated efficacy in augmenting glycolysis by activating an initial ATP‐producing enzyme in the glycolytic pathway, thereby increasing intracellular ATP levels, and exhibiting potential therapeutic effects in diseases such as Parkinson. Increasing ATP could play a role in retarding cellular ageing, as well as enhancing the activity of endothelial nitric oxide synthase to facilitate the release of nitric oxide and vasodilation.
Considering the association between vascular stiffness and metabolic inflexibility, similar to the ageing process, we hypothesised that Terazosin may also have efficacy on anti‐vascular stiffness. Therefore, we conducted a pilot study to investigate the effect of low‐dose of Terazosin on the improvement of arterial stiffness.
To minimise adverse effects from blood pressure reduction, we employed low doses of Terazosin (0.5 mg or 1.0 mg/day) to investigate its blood pressure‐independent positive impact on vascular stiffness in middle‐aged and elderly human subjects.
We compared the Terazosin study with previous reports on antihypertensive drugs. Previous research has shown that elevated arterial stiffness can precede the onset of high blood pressure, highlighting the importance of intervening in vascular stiffness even in non‐hypertensive patients. Our findings revealed that Terazosin significantly improved vascular stiffness in both groups, with consistent trends observed in blood pressure changes and arterial compliance improvements attributed to the medication. No adverse effects from excessive blood pressure reduction were observed, indicating its safety and efficacy.
No heterogeneity was observed in the risk for vascular improvement non‐response with varying doses of Terazosin usage, suggesting that lower dose (0.5 mg/day) Terazosin treatment remains effective.
If confirmed by larger trials, good to know that even 0.5 mg/day can improve arterial stiffness @DrFraser:
Overall, doxazosin had higher incidence of side effects than alfuzosin, which in turn had higher incidence than prazosin, tamsulosin, and terazosin; the latter three were not different from one another in rates of overall side effects. Alfuzosin was more likely to cause a fall than any other alpha blocker.
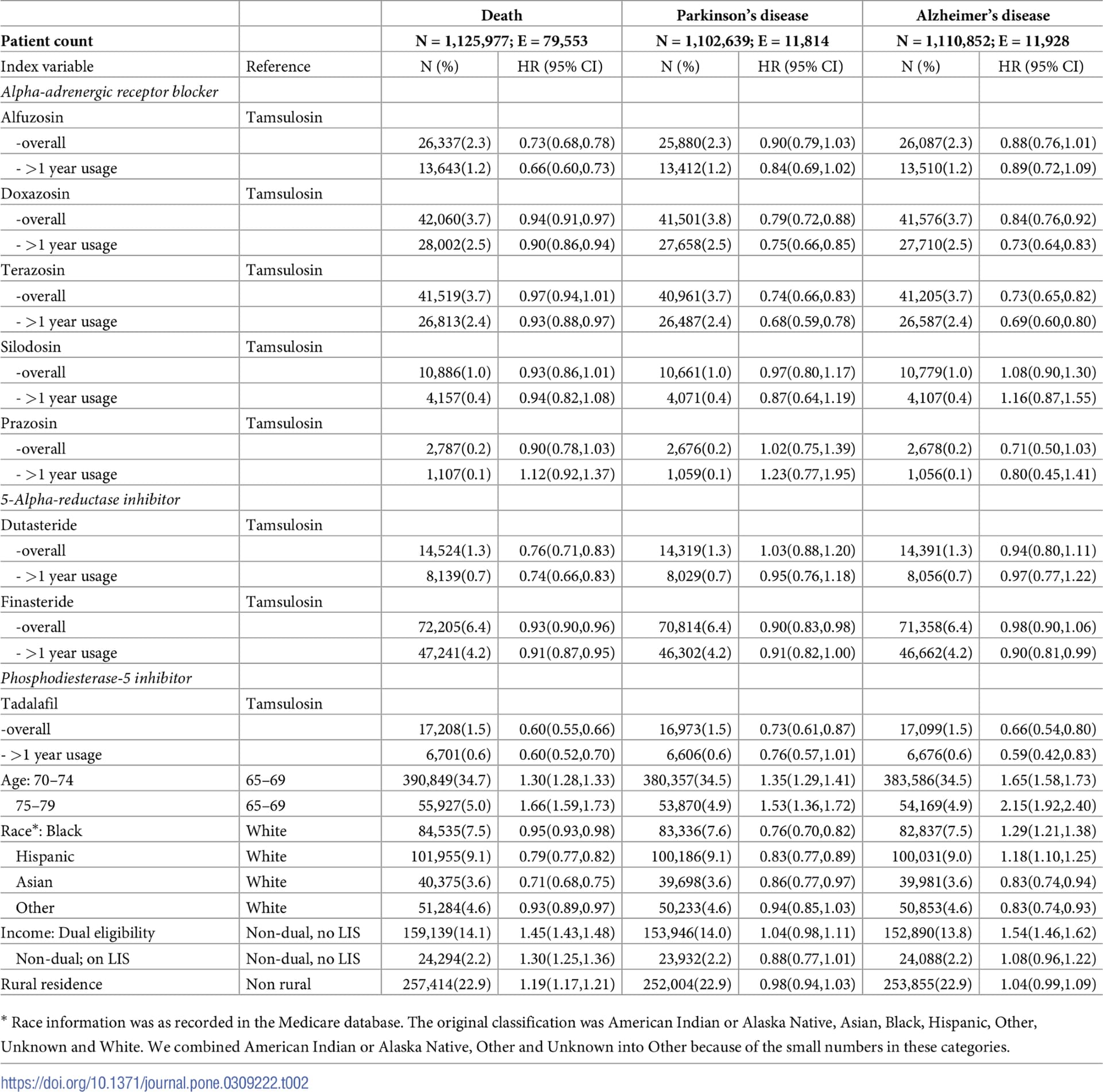
The study analyzed 1.1 million patients for a mean follow-up period of 3.1 years from being prescribed one of the study drugs. For all outcomes, patients on tamsulosin were used as the reference for comparison. For mortality, alfuzosin was associated with 27% risk reduction (HR 0.73, 95%CI 0.68–0.78), and doxazosin with 6% risk reduction (HR 0.94, 95%CI 0.91–0.97). For Parkinson’s disease, terazosin was associated with 26% risk reduction (HR 0.74, 95%CI 0.66–0.83), and doxazosin with 21% risk reduction (HR 0.79, 95%CI 0.72–0.88). For Alzheimer’s disease, terazosin was associated with 27% risk reduction (HR 0.73, 95%CI 0.65–0.82), and doxazosin with 16% risk reduction (HR 0.84, 95%CI 0.76–0.92). Tadalafil was associated with risk reduction (27–40%) in all 3 outcomes. More research is needed to elucidate the underlying mechanisms of these observations. Given the availability of safer alternatives for treating benign prostatic hyperplasia, caution should be exercised when using tamsulosin in elderly patients, especially those with an increased risk of developing neurodegenerative diseases.
Tamsulosin seems to be a terrible drug that should be avoided at all cost. Among alpha blockers, terazosin seems best for neuroprotection and it’s also safer (paper above).
Tadalafil is interesting but I can imagine many biases. Also, the 1y use OR is not lower compared to any use, which suggests potential biases. For alpha blockers it is lower.