There’s some evidence that it might slow down cognitive decline in people with T2D (9,901 participants, 371 sites, 24 countries, -14% “substantive cognitive impairment” per year?):
So, it’s not obvious that dulaglutide is better than liraglutide based on the above. But it might be easier to lower the decline in people who already have AD than to prevention dementia onset on people who are at risk (T2D) but still cognitively healthy.
The researchers gave normal mice the drug nivolumab/relatlimab, a melanoma medication that contains a Lag3 antibody, and found that it also stopped Aplp1 and Lag3 from interacting, again almost completely blocking the formation of disease-causing alpha-synuclein clumps in neurons.
The results reveal that Lewy bodies develop only when dopaminergic neurons are exposed to both a rise in alpha-synuclein and an immune stimulation. Without the immune challenge, no Lewy bodies developed.
Moreover, performing the same procedure on other cells, such as cortical neurons does not produce Lewy bodies, suggesting this effect is specific to dopaminergic neurons.
By following the development of Lewy bodies in real-time, the scientists discovered that in dopaminergic neurons, the immune response impairs autophagy—the removal of damaged cellular materials.
“Future studies should focus on understanding how inflammation caused by an overexcited immune system causes Lewy body formation when coupled with α-synuclein.”
Findings may guide future Parkinson’s treatments focused on immune modulation.
So, if this paper is correct, then curing Parkinson’s and Lewy body dementia would require both increasing autophagy and lowering the immune response. Obviously, rapamycin comes to mind… Unfortunately, the paper states that this is true for dopaminergic neurons only so we need a brain penetrant sirolimus-like… tacrolimus or everolimus?
The study team is now working to understand the disconnect between the encouraging phase 2 results with exenatide, the clinical success in Parkinson’s patients of another GLP-1R agonist lixisenatide, and these new phase 3 results with exenatide. They also are working to identify all learnings from this trial to inform future research in the GLP-1 field and beyond. Results of two sub-studies, funded by Cure Parkinson’s with Van Andel Institute, are still forthcoming as well, which sought to gather additional evidence on how the drug interacts with cells and whether a wearable device and smartphone app can be used to help track motor symptoms.
There is a thought that if Parkinsons is caused by mitochondria being damaged and mitochondria are damaged by high glucose then anything that keeps glucose under control would be good for parkinsons.
The difficulty, however, is that keeping glucose under control does not necessarily lead to improving mitochondrial function.
This might explain why in a previous trial another GLP-1RA failed but looking at “young” people (less than 60yo) it succeeded. It might be that passed a certain point of no return/damage, lowering glucose is not enough.
And you might need to ask on several pathways at the same time. Such as GLP-1RAs and/or SGLT2i for glycemic control and urolithin and/or rapamycin for mitochondrial function?
To my blinkered eyes Parkinsons looks like another disease of aging.
I have, in fact, just emailed cureparkinsons so see if they have any people interested in biohacking solutions such as the ones we normally talk about.
Interesting - and yes, these meds, including rapamycin seem much better at preventing rather than reversing. In early disease I think we have some hope still, especially in my patients who are in their 50’s, as we are getting access to compounded dulaglutide so it can be done for <$120/month.
Wait…dulaglutide? I thought you preferred tirzepatide, because of the GIP.
Anyway, I’m struggling to convince myself the last few pens of exenatide are worth taking now, after the study results. Thought I’d try tirzepatide. But the problem with all these “slow/halt the progression” treatments is that “slowing/halting” of anything is hard to measure, especially in my N of 1 experience.
I suspect we will find separate additive benefit from GLP that gets into the brain having GLP activity in the brain, which is different from the functional changes seen powerfully through signaling from the vagus nerve, which the newer agents are more potent for.
I’m favoring a dulaglutide and tirzep or retatrutide blend to hit GLP through both ways.
I have access to this compounded upcoming on the dulaglutide and the others.
Apolipoprotein B, low-density lipoprotein, and total cholesterol reduce PD risk, while homocysteine increase PD risk.
Apolipoprotein A1 is a protective factor for AD, while homocysteine is a risk factor for AD.
Based on other MR studies, ApoB, LDL and TC are probably causal for PD, while Hcy is not.
So PD is really the disease of healthy people: smoking, dyslipidemia, diabetes, obesity, poor diet, and television are protective while intelligence and high income are risk factors
At a dose of 200 mg once daily, “all the biomarkers and all the clinical and cognitive outcomes were moving in the correct direction,” Turner reported.
Nilotinib was safe and well tolerated, with more adverse events noted in the placebo group (74 vs 37; P = .54). There was an increase in the levodopa equivalent daily dose in the placebo group, but no significant increase or no change in the nilotinib group, which would suggest more parkinsonism or disease progression in the placebo group.
Notably, Turner added, there were fewer falls in the nilotinib group than the placebo group (6 vs 21) — a “70% reduction,” which could be due to improved cognition with nilotinib.
This is amazing. Has there ever been a successful phase 2 trial for LBD? It might be a first! Can’t wait for the phase 3! How safe is nilotinib? Can it be used for “longevity” / “neuroprotection” purposes @DrFraser? I’ll sponsor nilotinib in C. Elegans and see…
In clinical studies, the use of nilotinib in PD has so far yielded inconclusive results. A trial in 75 patients with PD randomised to receive placebo, nilotinib 150mg or 300mg for 12 months showed that nilotinib is safe, well tolerated and can increase dopamine metabolites in the CSF as well as reduce CSF α-synuclein oligomers and hyperphosphorylated tau [50]. An open-label extension of this study that included 63 patients for an additional 12 months randomised to receive 150mg or 300mg nilotinib showed that nilotinib continued to be safe and tolerated and demonstrated that nilotinib 300mg was associated with stable scores in the Movement Disorder Society Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) from baseline to 27 months in parts I (nonmotor including cognitive) and II (activities of daily living), while nilotinib 150mg was associated with improvement in the sum of UPDRS Part I (nonmotor including cognitive) and II (activities of daily living) with no difference in the UPDRS Part III (motor examination) [51]. Quality of life measures also worsened in the nilotinib 150mg compared to 300mg group between 15 and 27 months [51]. However, another double-blind placebo-controlled study that enrolled 76 patients with PD who received nilotinib 150mg or 300mg or placebo for 6 months showed that, while nilotinib was safe and well tolerated, patients in the nilotinib arms showed worse motor scores (measured with the MDS-UPDRS) [52]. This study failed to identify any changes in the dopamine metabolites in the CSF and suggested that, at least for PD, there was no evidence to support further testing of nilotinib.
Other ongoing trials of drugs from the same family (or related):
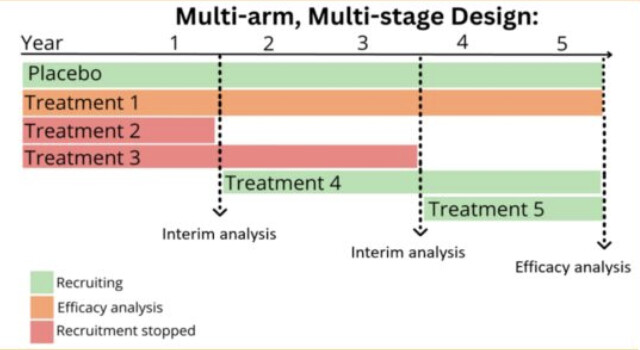
They’re starting a multi-arm, multi-stage (MAMS) trial platform in the UK to accelerate research: one shared placebo arm to lower cost and lower the % of participants with placebo (to increase the willingness to join the trial) + continuous assessment and if one treatment doesn’t work it’s directly replaced by the next candidate in a ranked list of compounds:
Did you mean 250 mg? The dosing for gallstone prophylaxis is 600 mg a day, and dissolution is 8 - 10 mg/kg/day.
I’ve been looking into TUDCA which is the same but taurine attached, and OTC, because I think I have gallstones and I would guess it’s good to try and dissolve them (because my ALP is high - higher ALP associated with higher ACM). 1 in 7 have asymptomatic gallstones.