(edit: I found a better description of this research)
This study (2021) found Parkinson’s patients have higher levels of Klotho in Cerebral Spinal Fluid (CSF) and lower levels of Klotho in their blood than controls.
In PD patients, Klotho in the CSF and alpha synuclein were inversely correlated: more Klotho, less damage.
If I recall correctly, Dena Dubal (Klotho researcher) notes that Klotho does not cross the BBB in the Peter Attia interview, but she says it has a lasting effect on brain function for primates regardless.
Yeah we’ve gone over that before. Statins are either negative or neutral for PD risk, as well as other lipid lowering treatments are probably negative, but I’m unsure how to weigh PD risk vs. CVD risk, if someone has a family history of the disease.
According to the data, it appears—in principle—to be possible to stop, if not reverse the progression of Parkinson’s disease in the prodromal iRBD-stage.
They used 5 g/d of acetyl-DL-leucine (ADLL, also called acetylleucine):
ADLL is commercially available under the trade name Tanganil® in France. It has been registered for the indication “vertigo” since 1960. The drug contains the racemate of acetyl-leucine, i.e., the inactive D-form and the bioactive enantiomer, the L-form of acetyl-leucine in equal parts.
[EDIT: “patient 1 showed a trend of decrease in the MoCA score and developed a mild cognitive impairment during the study” and the MoCA scores decreased… ]
Tanganil is sold OTC in France.
N-acetyl-L-leucine looks more potent (and safer?) than ADLL, and is developed by IntraBio as IB1001. IntraBio applied this year to the FDA for Niemann-Pick disease type C (NPC).
The mechanism of action is unclear. The authors write:
Acetyl-leucine (AL) has been found to have symptomatic and disease-modifying effects in animal models of lysosomal storage disorders (LSD), including Niemann-Pick disease type C (NPC) and GM2 gangliosidosis. Several formal LSD clinical trials with the active L-enantiomer, including our recent double-blind, placebo-controlled crossover phase 3 trial in NPC8, found that N-acetyl-L-leucine had rapid beneficial effects on neurological signs and symptoms and an excellent safety profile. The agent enters enzyme-controlled pathways that correct metabolic dysfunction and improves energy adenosine triphosphate (ATP) production. Lysosomal and mitochondrial dysfunctions have been proposed as important factors in the pathogenesis of PD. Therefore, AL might also have a favorable impact on the prodromal stage of PD by slowing down its progression already in the stage of iRBD.
Yes that’s why I’m using ezetimibe and not a statin. There’s also the paper showing reduced PD risk with ezetimibe. Not super strong evidence though, but still better than statins that are definitely shown to be detrimental in PD.
You know, I keep hearing about this, but I really do wonder how strong the evidence against statins is wrt. PD. The other day, I came across a very interesting paper, well worth reading:
Very strong: RCT + association studies + Mendelian randomization + potential mechanism (messes up with GLP-1 in the gut). Everything is in this thread.
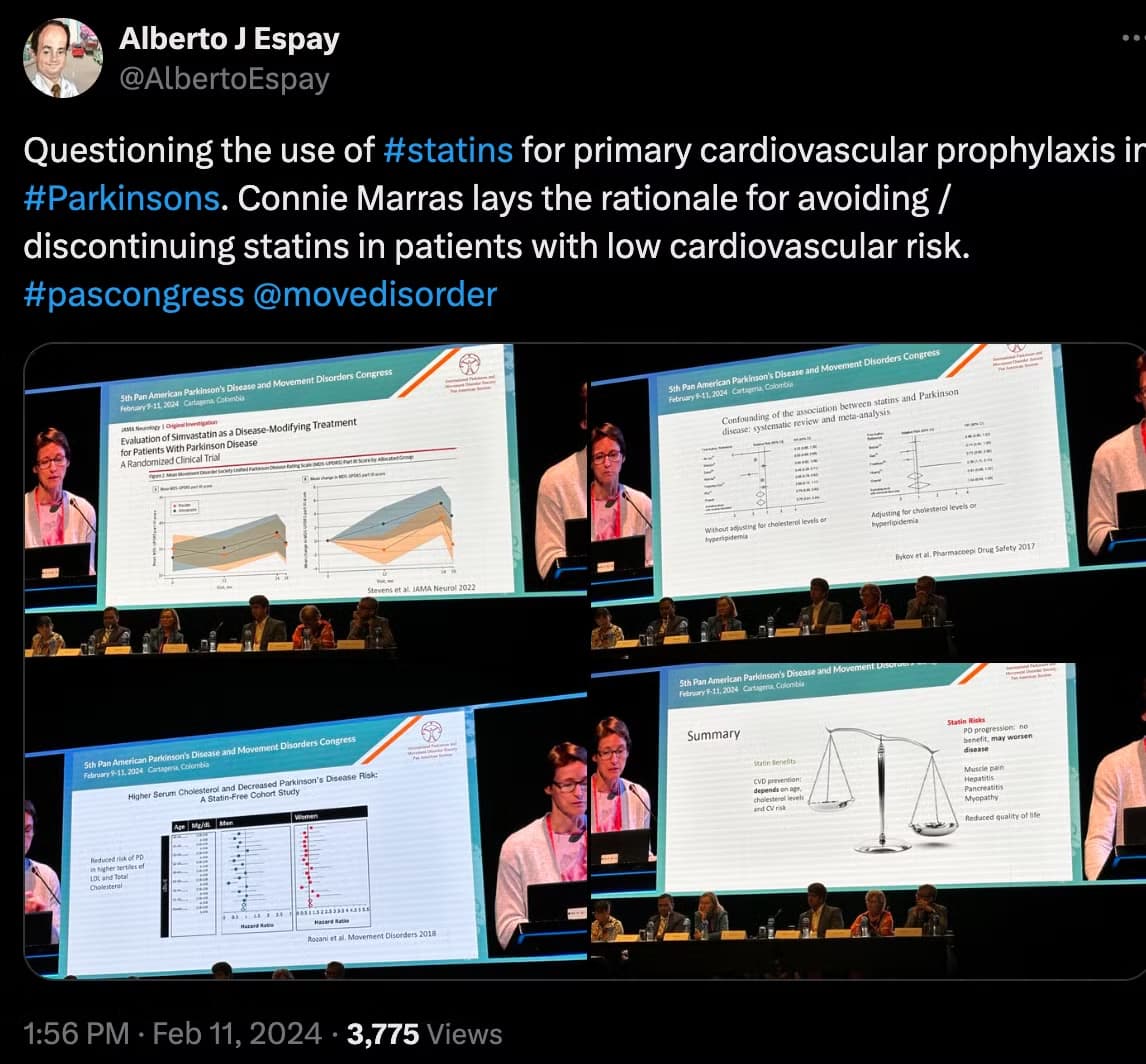
Some earlier papers suggested a potential protective effect, but I think now the mainstream view is that statins are neutral at best. And some serious PD researchers and neurologists are advocating for statin discontinuation in people with PD. For instance, Connie Marras, Professor of Neurology at the University of Toronto (on the Scientific Advisory Board of the Michael J Fox Foundation and the Parkinson’s Foundation):
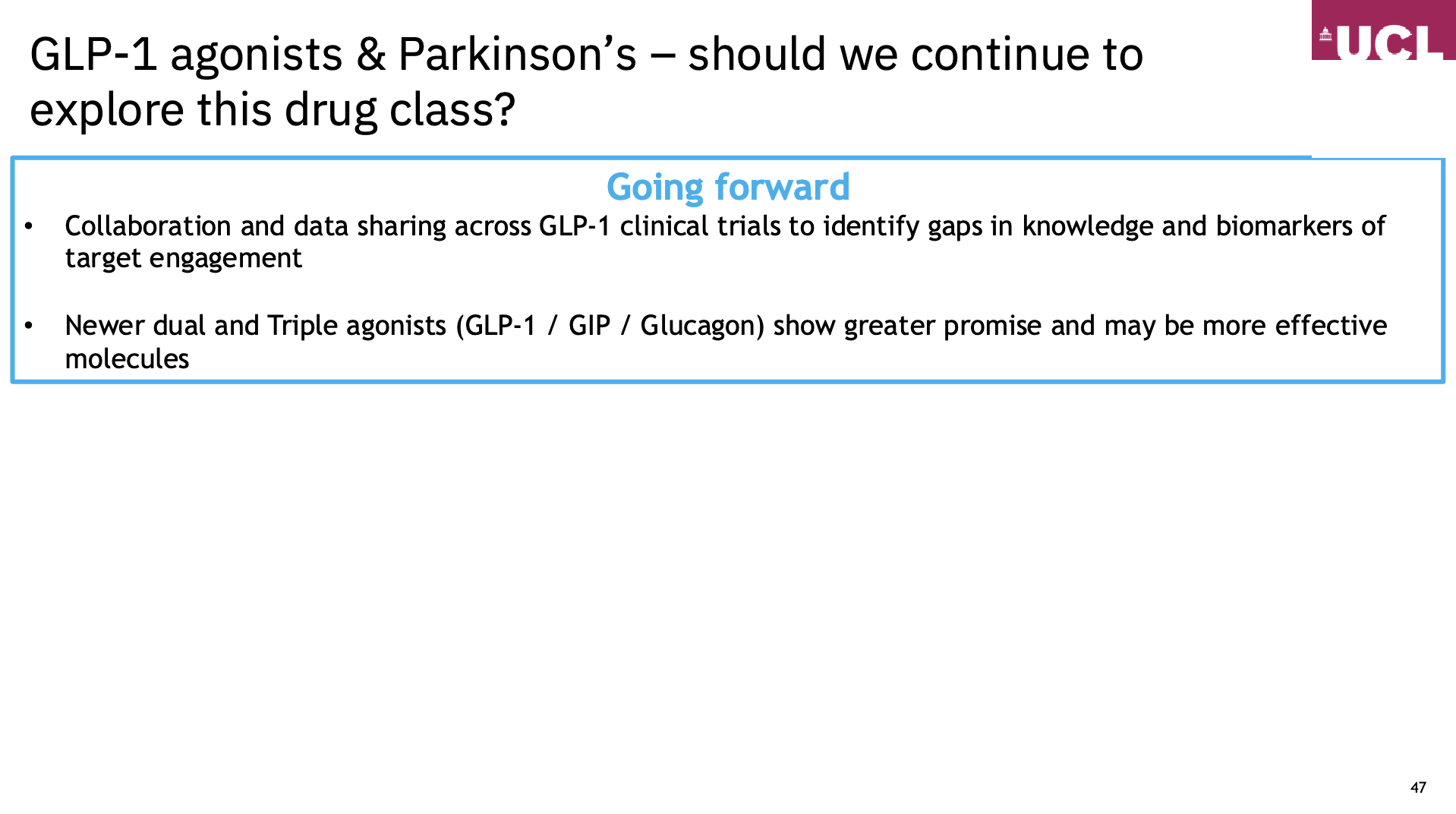
It’s very interesting that the speaker concludes “Newer dual and Triple agonists (GLP-1 / GIP / Glucagon) show greater promise and may be more effective molecules” as he is behind the exenatide trial and as of 2022 he was exploring dual agonists (but nothing published yet?): Diabetes dual agonist drugs for Parkinson's - Cure Parkinson's
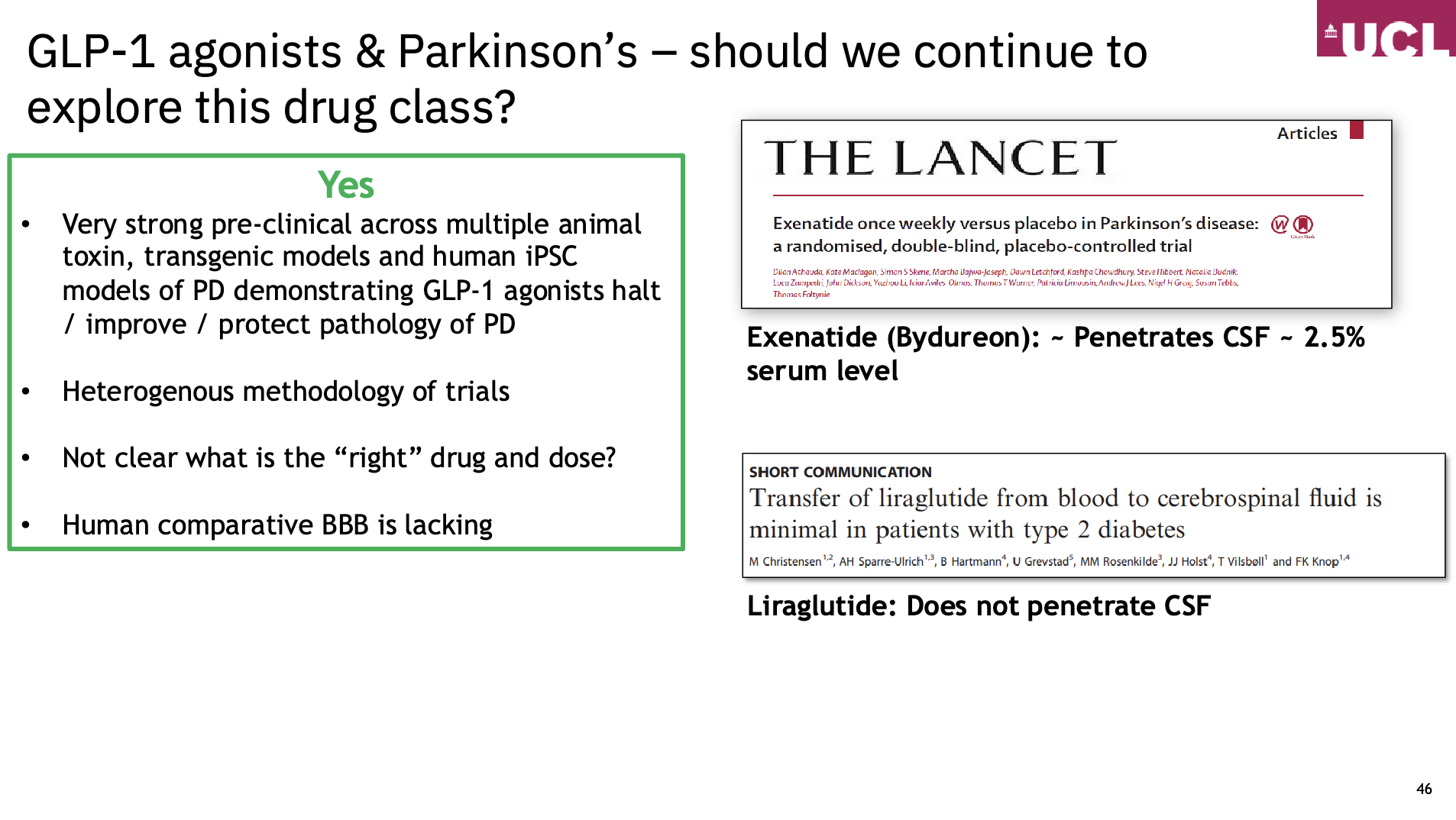
I assume that the best would be a BBB-crossing triple agonist. But today, we have to choose between BBB-crossing single agonists (exenatide, lixisenatide, dulaglutide) and dual or triple agonists that don’t cross the BBB (tirzepatide, retatrutide?)…
Excellent presentation - really would like to see more on Semaglutide and Tirzepatide due to their potency, but also with the lack of BBB penetrance. I’m a bit surprised that the producers of Semaglutide and Tirzepatide aren’t funding a decent sized study on this issue as it would get them yet another valid indication, evidence based for their drugs which are quite expensive.
The anti-inflammatory effect might also explain how GLP-1 drugs help to ease the symptoms of neurodegenerative diseases such as Parkinson’s4,11 and Alzheimer’s disease. Approved drugs for the conditions don’t target the excessive brain inflammation that is characteristic of these diseases.
Christian Hölscher, a neuroscientist at the Henan Academy of Innovations in Medical Science in Zhengzhou, China, says that the clinical evidence on the utility of GLP-1 drugs in Parkinson’s is already compelling and that, if positive, the phase III trial results for exenatide will be a game-changer for clinical practice. Hölscher is the chief scientific officer of Kariya Pharmaceuticals, a Danish biotech firm in Copenhagen that is exploring GLP-1 drugs as a way to treat neurodegenerative diseases.
He is now working on strategies to develop GLP-1 drugs that penetrate the brain in higher concentrations than for currently available drugs. “There’s a clear correlation between the ability to get into the brain and the neuroprotection effect,” he says.
A similar mechanism could explain some promising preliminary results for Alzheimer’s disease, too. Hölscher’s colleagues presented a small, unpublished study at a conference in July suggesting that cognitive decline in people with Alzheimer’s who took liraglutide was 18% slower over a year compared with those who were given a placebo.
Semaglutide is also being evaluated for treating early Alzheimer’s disease in two large clinical trials sponsored by the drug maker Novo Nordisk, based in Bagsvaerd, Denmark.
I think the article specifically shows the opposite. It’s NOT that people with PD have too little uric acid:
The discovery that energy metabolism is disrupted in PD opens the door to new treatment strategies. Current therapies largely focus on managing symptoms, but this research suggests that targeting the body’s energy recycling system could slow the disease’s progression. This study shows that treatments aimed at elevating serum uric acid levels might have limited efficacy in improving Parkinsonism. Instead, focusing on the purine recycling system, particularly enhancing ATP production, could hold more promise.