I’ve created a first draft of a simplified spreadsheet for tracking the elimination half-lifes of Rapamycin and Everolimus.
The goal of this spreadsheet is to help us understand what the optimal dosing schedule might be for our own doses we are taking. Ultimately we’ll probably want to start doing Blood/Sirolimus testing at the trough (the day before we take the next dose) to see what our actual blood sirolimus levels are prior to the next dose. This will help us understand our potential risk for longer term side effects (it seems). But in the shorter term, this type of spreadsheet might help us understand the timing of the dosing that might work best for us.
Given the ranges of drug elimination half-lives that are reported in the research literature (older, sicker patients seem to have shorter half-lives from my initial inspection of the data) this isn’t that specific, but its a start.
The general goal as suggested by the geoscientists and medical doctors focused on this topic seems to be that we want to make sure we get the trough levels (the lowest levels of the drug before the next dosing) down quite low. The exact definition of “low” seems to be rather vague from what I’ve seen - and in fact not well understood or researched yet, and ultimately “low” is based on blood levels of rapamycin or everolimus - which most people are not testing right now. I’ve heard Dr. Green sets a target of 5 half-lifes (lives?) for his once every two week, 20mg dosing schedule.
Generally the scientific literature strongly suggests that the lower the trough levels, the lower the side effects (and thus one of the rationales of periodic “rapamycin vacations” of being completely off the drug - so any potential more serious side effects are avoided).
Your comments and thoughts are welcome. See google spreadsheet below:
To me, this makes a strong argument for higher dosing fortnightly rather than lower dosing weekly: the troughs are much deeper and there are potential benefits of the higher dosing in pentrating the blood-brain barrier. I have not tried this yet.
Yes - I tend to agree. It also seems to suggest that everolimus at higher doses might be more effective than rapamycin / sirolimus , or at least cause fewer side effects for a given dose level.
This entire issue seems to warrant a lot more investigation … I’m going to be interviewing the lead author on the 60% lifespan increase w/rapamycin paper next week. Add any questions you can have to that post…
I’ve thought about this but it’s really interesting to see on a spreadsheet. Wondering how much diet (ie…fat, grapefruit juice, and supplements like tumeric, piperine, etc.) impacts the “average” as well.
I thought that the dietary additions, used prior to or with rapamycin, acted by increasing absorption. That would imply an equivalent higher dose but a similar half-life. If I am wrong, and the diet can also decrease breakdown, then the half-life might be affected and might continue to be affected by subsequent meals.
I hope the 60% lifespan result can transfer to human, and would like to know what’s the reasonable dose to try, if we want to get approximately the same effect in mice
But the concern is if the high dose intermittent regimen hurts reproductive system?
There are researches shows continuous high dose of rapamycin may hurt gonadal function
…and decreases sex hormone
But there also is a research in mice suggests rapamycin may improve erectile function
Waiting for the interview, and appreciate your work
Made some calculations:
20mg every 2 weeks when half-life is 72 hours, gives close to 0.8 mg at trough.
5 mg every week when half-life is 72 hours, gives close to 1 mg at trough
@shc yes - those trough levels look good, though I’m not sure there is any research telling us what we should be shooting for in terms of trough levels prior to the next dose. Of course there are significant individual variations in the half life… depending on age, food, other medications, etc…
Also - the 20mg/week level of everolimus/RAD001 was already tested in the Mannick trial and the side effects don’t look that bad from what I can tell. But its hard to know how to interpret the side effect results - does the 17% reporting headaches (for example) represent people getting a headache once for a short period of time and then it going away, or was it a more persistent problem… it would be nice to have more data.
I interviewed Alessandro Bitto, the lead author on this paper on Monday - where they tested the high dose of the equivalent dose of 378ppm per day in mice for three months (and then stopped and let the mice life out their lives) - and it extended the remaining life expectancy (the mice were already the equivalent of 60 years old) by 60%. This suggests to me there may be some upside to higher doses.
Its frustrating that more clinical trials are not being done on rapamycin right now… so much more data is needed.
The research strongly suggests that the negative impact on sperm production is only temporary and goes away once the rapamycin is stopped or paused. We cover it here in this section of the website: Rapamycin risks in healthy adults.
Also - it looks to be the same type of thing that happens with caloric restriction (another well-proven approach to life and health extension). In fact caloric restriction and rapamycin/mtor inhibition have been proven to overlap a great deal. It seems to be an evolutionary adaptation - when your body doesn’t think it has enough food/energy having babies is probably a bad idea - so it shuts those functions down until things get better.
The same thing happens when people get in extremely good physical shape, with very low body fat, and who exercise at very high frequency and levels.
The whole point is that rapamycin tricks the body into thinking that its nutrient starved (mTOR is the nutrient sensing pathway, that is blocked with rapamycin) and this causes your body to shut down extraneous functions that are not absolutely needed in a low nutrient environment (like making lots of sperm and having babies).
As they say in the second paper listed below:
Our hypothesis was supported: nutrient restriction of pre-pubertal rats delayed reproductive development, induced negative energy balance and decreased metabolic hormone concentrations (commensurate with restriction), whereas short-term refeeding after profound restriction largely restored reproductive end points and plasma hormone concentrations, but not body composition.
If one is dosing weekly, there is never any total wash out. And even biweekly dosing also never washes out completely between doses. Is there a good reason to abstain from sirolimus/rapamycin for an entire month in order to clear it to near zero?
Good question, but there is a real lack of information and research around this right now - we really don’t know. To be safe on the safe side it seems like a good idea to periodically take a rapamycin break for 1 month+. Here is Dr. Peter Attia’s protocol, the last time I heard about it:
By the way - My belief is that Dr. Green does not have his patients do any rapamycin vacations to clear any inhibition of mTORC2 that may be happening.
I believe @AgingHippie is a patient of Dr. Green’s and perhaps he can either confirm or correct me on this issue.
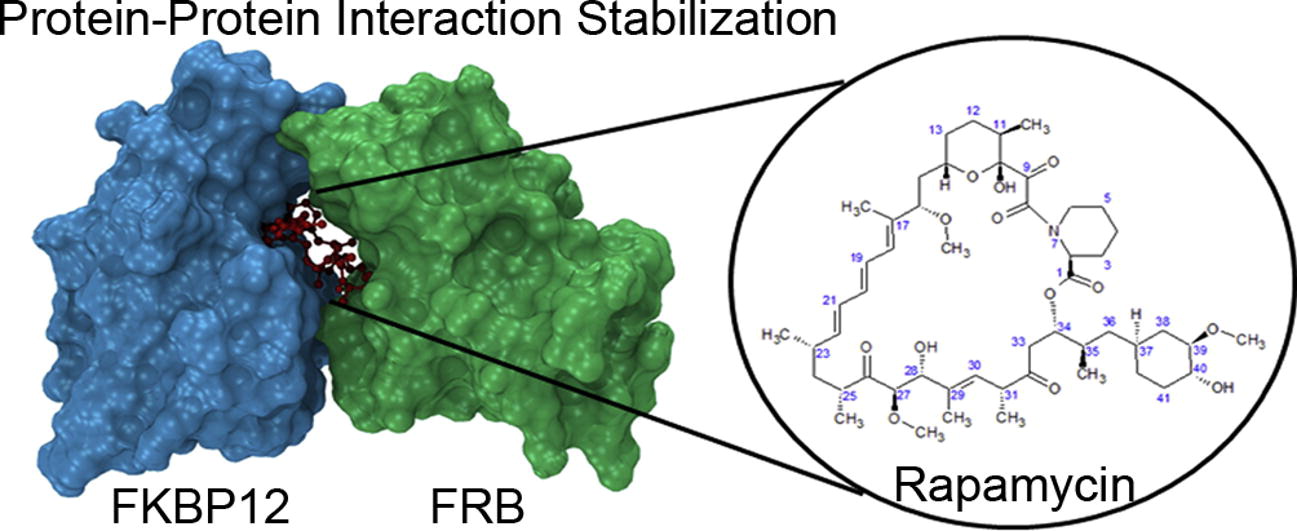
Looking at the molecular structure, rapamycin is like a key inserted into a tiny keyhole between two large proteins FKBP12 and FRB. I wonder how rapamycin can dislodge/wash out from this tight combo once its bonded together. If you look at 2016 mouse trial report, its still effective six month after termination of dosing.
I have not looked closely at the molecular structure - where did you see that described in detail (which paper was best for this?). Would this explain the long half-life of the drug also? Could you give me a link to the 2016 mouse paper you mentioned?
Oh yes - that mouse paper. I interviewed the lead author on that paper (Alessandro Bitto) last Monday. I’ll try to publish the transcript next week.
Yes - very interesting. 3 months of a very high dose of rapamycin (equivalent to 378ppm), gave almost the same lifespan increase as taking a lower dose (42ppm) from 20 months to end of life.’
The whole dosing schedule / level issue is so interesting and needs some really good studies to tease out the optimal approach… this is something that could be ongoing for the next decade I suspect.
It doesn’t keep building up. I ran into this question a couple of years with some other prescription drugs. Assuming 80 % cleared in a week, right after second week dose you have 6mg plus 1.2 mg of the first week dose, or 7.2 mg in your system. However, in the coming week 80% of 7.2mg is cleared. If you do a spreadsheet you see that the level peaks at 7.5 mg right after your weekly dose and a minimum of about 1.5 mg in your system just before a new week’s 6 mg dose. The big unaswered question though is: Do we want this??? Would we be better off with a day or more of total clearance? Hopefully we will have answers in the not too distant future.