@RapAdmin I have not! I will do that now.
Thank you very much:)
No, but its highly personal in terms of response
Be sure to read the rapamycin FAQ at the top of the page in the header of the site.
Rapamycin is keeping lipids out of your cells so your blood levels are going up. That’s why we coat stents with rapamycin.
RapAdmin, curious to hear your reasoning for returning to weekly dosing from biweekly.
You know… I don’t see much difference between the two (from a data perspective - though obviously more data on the weekly side because we have the Mannick papers on weekly) and I tend to find it just a little bit easier to follow a weekly schedule.
I think my next tweak on my dosing will be to alternate between everolimus and rapamycin / sirolimus on a week by week basis, due to the potential BBB benefits.
Thank you, RapAdmin. Just out of curiosity, did you notice any changes to your lab results (positive or negative) after doing the the higher dose biweekly protocol?
Hi Basil,
Welcome to the group. there is a vast amount of information here. One thing that I have not seen mentioned is rapamycin and reproductive capacity. As your photo shows you to be a relatively young woman, you should read up on what rapamycin’s effects on sex hormones are and include those in your blood tests. Basically, rapa is NOT recommended for anyone planning on having children in the future, both male and female. It shuts down sperm production in men and reduces production of estrogen and testosterone. Here is one study
Now for older people, this may be a good thing. The hypothesis is that the reason women tend to live longer than men is that menopause dramatically reduces estrogen production while men keep producing testosterone as they age. Sex hormones raise Mtor, which may be why lower sex hormones leads to longer life.
On another topic, I understand your concern about metformin but I think it is overblown for older people. Remember, the goal here is increasing life span by increasing health span. Aging is caused by age-related disease like cancer and artherosclerosis. One reason to take metformin is to lower blood glucose, but another, more important reason is that people who take metformin are much less susceptible to cancers (though it is still unclear if this is causation or merely association). I take metformin and exercise daily without side effect. I’ve never heard of metformin causing insomnia but ou might try taking it in the morning. Another drug that can reduce glucose is acarbose, which blocks digestion of carbs in the gut. Talk to your doctor about borderline blood tests for H1AC and LDL. A better test than LDL is for Apolipoprotein B.
Hi @Uppereast69 , thank you for the compliment:) - I am actually 55YO and that photo was taken 5 years ago when I was 50YO.
I’m in menopause so I don’t think I have anything to worry about there.
But I do appreciate you providing all of this information.
Regarding metformin, I always took it in the morning and started on 500mg. It made no difference. The effect that I was wide awake for most of the night, tried for 3 nights and then gave up.
I was most disappointed as I had heard good things about it.
I guess my body says it’s not for me.
The best age to start rapamycin is still very much an open question in humans - some, like Dr. Blagosklonny, think the right age is younger - around age 25 but others think later. Possible risks (that are seen in high-dose, continual dosing, applications like organ transplant patients and cancer, or high-dose mouse studies) are covered in this section of the website: Possible risks of rapamycin in healthy humans.
Regarding menopause - we have had people using rapamycin that say their menopause is reversed with rapamycin:
Please let us know if you see any results like this.
Will do:), though I doubt it because I am taking bio-identical HRT to help with the debilitating symptoms of menopause such as insomnia.
Perhaps aim for 0.1mg/kg. I weigh 74kg and take 8mg but if you weigh 56kg you might only want to take 5mg…
Also, if you’re concerned about sleep take it (with some olive oil) on waking as many people get a slight stimulant effect.
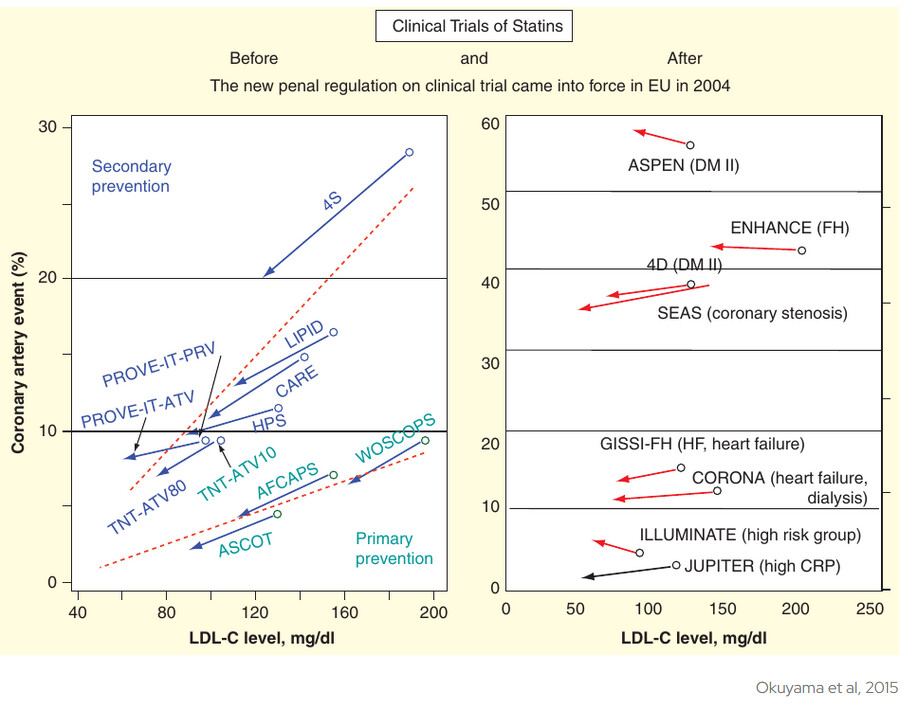
Before jumping back into statins
After the instantiation of new reporting rules in 2004 [requiring disclosure of conflicts of interest], all clinical trials demonstrating that statins reduce LDL have shown no significant benefit for prevention of CHD.
This chart of research results is through 2015, so are there more recent studies pro or con, or did they miss any?
Sorry, I don’t give much credence to articles like this. There are many peer-reviewed studies that refute his opinion.
If you’ve never had a heart attack, and you have no other risk factors, no smoking, hypertension, diabetes, or a strong family history, then your heart attack risk is very low . Intervening with a statin to go from low risk to low risk is just putting yourself at risk for myopathy, diabetes, and heart failure, with little to no gain.
Is there a peer reviewed study that refutes this statement with strong evidence that was reproducible?
Just saw this new paper…
It’s starting to look like everything is related to the gut microbiome. That’s something that we’ve really been neglecting.
Well, first produce your own large-scale peer-reviewed study that supports Remnantl MD’s supposition.