In a landscape saturated with “anti-aging” supplements, a new review by researchers at the Medical University of Graz provides a sober, clinical audit of the most hyped molecules in longevity: NAD+ precursors. Nicotinamide Adenine Dinucleotide (NAD+) is the cellular fuel that powers mitochondrial engines and DNA repair crews. NAD+ levels seem to go down in some tissues as we age (though results are inconsistent between studies) a decline linked to everything from heart failure to cognitive rot. For years, biohackers have popped Nicotinamide Riboside (NR) and Nicotinamide Mononucleotide (NMN) to reverse this, banking on spectacular lifespan extension seen in mice.
This 2025 review synthesizes the latest wave of human clinical trials to answer the trillion-dollar question: Does it work in humans? The verdict is a cautious “Yes, but…” While the safety profile is pristine—these compounds reliably boost blood NAD+ without toxic side effects—the translation to “feeling younger” is harder to pin down. The review highlights that while precursors successfully engage their targets (elevating the NAD+ metabolome), the downstream miracles—muscle regeneration, metabolic reset, and cognitive sharpening—are inconsistent across human cohorts. The authors argue we are moving from the “discovery phase” to the “precision phase,” where the focus must shift from if we should take them, to who should take them, when, and at what dose to bypass the bottlenecks of human metabolism.
Part 2: The Biohacker Analysis
Study Design Specifications
- Type: Systematic Review of Clinical Trials (Meta-Analysis context).
-
Subjects: Human cohorts from multiple Phase I/II trials.
- Populations: Healthy older adults, Obese/Overweight adults, Heart Failure patients, Acute Kidney Injury patients.
- N-numbers: Varies by trial (typically n=20 to n=100 per study cited).
-
Lifespan Data:
- Mice (Reference): Review cites rodent studies showing ~5-15% lifespan extension and improved healthspan.
Mechanistic Deep Dive
The authors dissect the NAD+ Salvage Pathway, identifying the critical failure points in aging:
- Supply Chain Failure: The rate-limiting enzyme NAMPT declines, preventing the recycling of Nicotinamide (NAM) back into fresh NAD+.
- Increased Burn Rate: Aging inflames tissues (Inflammaging), causing an upregulation of CD38 and PARPs. These enzymes voraciously consume NAD+ to fuel immune responses and repair DNA breaks, depleting the pool available for Sirtuins (longevity genes).
-
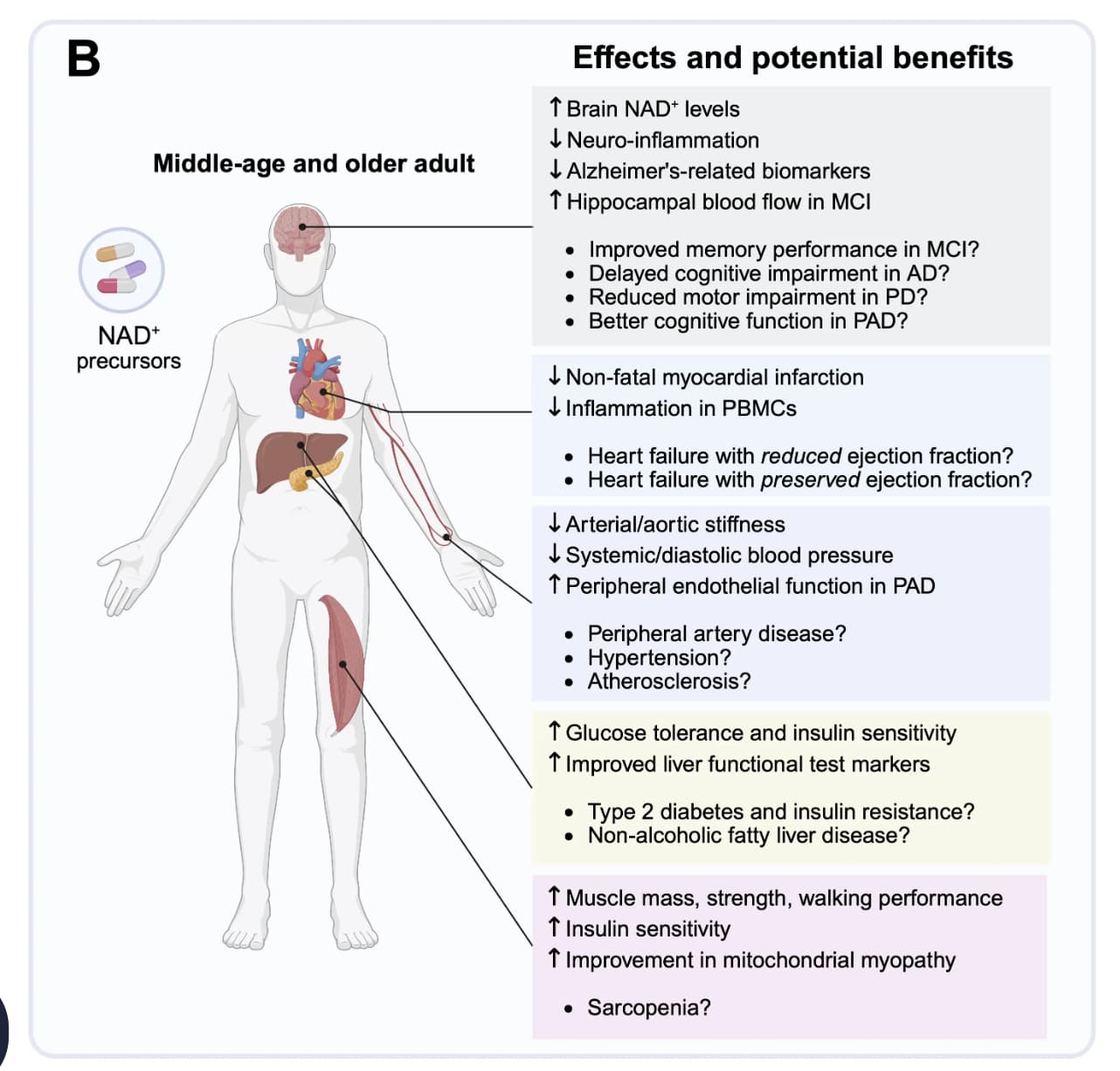
Organ Priorities:
- Skeletal Muscle: High sensitivity to NAD+ decline; supplementation shows potential to restore mitochondrial oxidative capacity (mitophagy).
- Cardiovascular: NAD+ is critical for endothelial health; depletion mimics heart failure energetics.
- Brain: Neuroprotection is the “Holy Grail,” but blood-brain barrier (BBB) permeability of precursors remains a key debate.
Novelty
This review distinguishes itself by aggregating the “second generation” of clinical data (2020-2025). Unlike early papers that just asked “Is it safe?”, this analysis focuses on tissue-specific bioavailability. It highlights that while blood NAD+ soars, muscle and brain increases are harder to achieve, suggesting that oral dosing protocols may need to be much higher or coupled with other agents (e.g., sirtuin activators like pterostilbene) to drive tissue uptake.
Critical Limitations
- The “Blood-Tissue Gap”: The review admits a major methodological weakness in the field: most trials measure NAD+ in blood (PBMCs), which may not reflect levels in the liver, heart, or brain. We are using a flashlight to look for keys in the wrong room.
- Heterogeneity of Response: There is massive inter-individual variability. Some subjects are “non-responders,” likely due to gut microbiome differences or baseline NAMPT activity, which few studies control for.
- Lack of Functional Endpoints: Too many trials rely on biomarkers rather than hard clinical outcomes (e.g., grip strength, VO2 max, cognitive scores), which often show no significant change despite elevated NAD+.
Context: Geromedicine, International (published by SciExplor), Vol. 1, 2025.
Impact Evaluation: The impact score of this journal is N/A (New Journal, Vol. 1), evaluated against a typical high-end range of 0–60+ for top general science, therefore this is an Emerging/Unranked impact journal.
Open Access Scientific Paper: Clinical evidence for the use of NAD+ precursors to slow aging