Testosterone for women (and men) is particularly good for muscle mass and bone strength. The main downsides are potential androgenic effects - hair growth, acne, deeper voice. At female dosing, there isn’t much serious downside. If anything, it would be CV risk but probably minimal.
Other positives are energy level, positive outlook, libido, etc.
Having looked at this for my wife for awhile, I think most post-menopausal women should be on what I term triple therapy - estrogen patch, progesterone pill at night and testosterone cream. Dosing mostly by symptoms but check testosterone levels to avoid going too high. I had a female patient with a 500 testosterone level from pellets. She had no downside but that is nuts. She reported anger issues only when she was low on T strangely enough. No voice changes either. She was 65 with a 50 year old husband …
Overall T is probably more health span than lifespan but fraility and broken hips kill so I think lifespan is likely improved also.
Now, there isn’t going to be any data particularly with starting later. With Estrogen, the thinking by many is that you shouldn’t start over 60 years old I believe.
Lastly, most studies demonstrate neuroprotective action particularly in cell cultures (of questionable relevance). But also in mouse models and some human disease states.
Jonas So, the doxycycline with the rapamycin has nothing to do with the combination of the two. It’s purpose is specifically for Alzheimer’s prevention. Or, did I misunderstand?
In my case I moved over to pitvastatin for its lower impact on insulin resistance. My LDL-C is down in the 40 range now, and so my priority is my slightly raised blood sugar levels: What's the best statin to take? - #51 by vishnu
These supplements may increase blood levels, and perhaps extracellular matrix levels, but the real question is do they increase intracellular NAD+ levels which is where an increased concentration of NAD+ could benefit us.
I haven’t seen any studies that suggest an increase in intracellular NAD+ levels. If you can reference, I’d be happy to take a look, but failing that, I regard these expensive supplements as a waste of money.
I use Magnesium L-threonate at night, Glycine in the morning, Malate if I am playing sports.
@KarlT I would love it if you could share your stack?
Any of my stack is non-sense that you want to tear up? I would welcome that. I am purposely stay “lean” for the time being and then add back some perhaps over time.
One thing I am adding this year is to use some of DORA sleeping medications to aid my maintenance sleep (Dayvigo 5mg) and better clearance of brain sewage at night. This is very recently discussed by Matt Walker (the sleep doc) and used by Tim Ferris etc.
On Doxy, it’s just I also have rosacea now and then so it’s part of insurance for a variety thing with me personally. I believe Peter Diamandis proposed Rapamycin with Doxy at one point.
I use it 100x twice a week as it is a dose that is not likely alter my gut bacteria.
Some of Gemini cited research on Doxy:
Key Researchers, Studies & Protocols
Dr. Johan Auwerx (2013/2022) | The Worm Longevity Model: Auwerx’s lab at EPFL established the foundational theory of “Mito-hormesis” by showing that doxycycline extends C. elegans lifespan by up to 70%. By mildly inhibiting mitochondrial ribosomes, the drug triggers a survival response called the Mitochondrial Unfolded Protein Response ($UPR^{mt}$), which effectively “tunes up” cellular repair mechanisms and reduces the accumulation of aging pigments like lipofuscin.
Dr. Baohua Liu (2024) | The Mammalian Breakthrough: Published in PubMed in 2024, Liu’s research moved the needle from worms to mammals by proving that doxycycline treatment extends the lifespan and rescues the physical decline in Progeria (accelerated aging) mice. The study highlighted that the drug works by suppressing IL-6 (a master cytokine of “inflammaging”) and preventing the breakdown of the nuclear envelope, a hallmark of cellular aging in humans.
Dr. Michael Lisanti (2019/2023) | The DAV Protocol: A pioneer in cancer metabolism, Lisanti developed the DAV Protocol (Doxycycline + Azithromycin + Vitamin C) specifically to target Cancer Stem Cells (CSCs). His research demonstrates that this triple combination “starves” the mitochondria of senescent and cancerous cells, preventing them from replicating and driving the metabolic decline that often accompanies advanced age.
Dr. David Sinclair / Life Biosciences (2025-2026) | The Epigenetic Remote Control: In a shift from using the drug as a supplement, Sinclair uses doxycycline as a molecular “on-switch” for gene therapy. In his current “rejuvenation” trials, patients receive a viral delivery of Yamanaka factors (OSK) that remain dormant until the patient takes a course of oral doxycycline, which activates the “cellular reset” to turn old, injured cells back into a younger state.
Jane McLelland & The Metabolic Community: As the author of How to Starve Cancer, McLelland has popularized the use of doxycycline as a Matrix Metalloproteinase (MMP) inhibitor. Biohackers in this niche use low-dose doxycycline to block the enzymes that degrade the extracellular matrix, aiming to preserve skin elasticity and prevent the systemic “leakiness” of tissues that occurs with age.
Based on the detailed clinical phenotype (High Risk CVD, APOE4 carrier, Metabolic Dysfunction, Osteoporosis), here is the prioritized, evidence-based ranking of the regimen.
Critical Safety Warning
Colchicine + Rapamycin Interaction: You are concurrently taking Colchicine and Rapamycin. This is a potentially life-threatening combination. Rapamycin inhibits P-glycoprotein (P-gp), which is responsible for clearing Colchicine. This can lead to toxic accumulation of Colchicine, causing severe myopathy, rhabdomyolysis, and multi-organ failure.[1, 2, 3]
Action: Given your high CAC and Lp(a), Colchicine offers proven mortality benefits.[4] Rapamycin is experimental. Prioritize Colchicine and pause Rapamycin until cleared by a specialist.
Tier 1: Essential “Standard of Care” (Keep & Optimize)
These interventions target your primary mortality risks (CVD, Metabolic) with high-quality clinical evidence.
Evolocumab (Repatha): The cornerstone for your lipid management. It is the only agent that aggressively lowers both LDL-C and Lp(a) while promoting plaque regression.[5, 6]
Bempedoic Acid + Ezetimibe: Essential non-statin backbone. Bempedoic acid avoids muscle side effects while effectively lowering LDL-C in statin-intolerant patients.[7, 8]
Colchicine (0.5 mg): Reduces cardiovascular events by ~31% in chronic coronary disease by dampening NLRP3 inflammasome activity.[4, 9]
Dapagliflozin: A caloric restriction mimetic. Reduces cardiovascular death and improves kidney function independent of diabetes status.[10, 11]
Testosterone (Transdermal): Critical for addressing “feeling meh.” Consensus guidelines support its safety for postmenopausal Hypoactive Sexual Desire Disorder (HSDD), muscle maintenance, and bone density.[12, 13]
Thyroid Support (T3/Synthroid): Non-negotiable for Hashimoto’s.
Tier 2: Targeted Geroscience (High Value)
Mechanistically sound interventions for your specific aging phenotype (APOE4, Muscle, Skin).
Lithium Orotate (Microdose 1-5mg): Superior neuroprotection for APOE4 carriers. Promotes autophagy and inhibits GSK-3β (a driver of tau/amyloid pathology) without the toxicity of high-dose carbonates.[14, 15, 16]
Urolithin A: Validated to improve muscle endurance and mitochondrial health (mitophagy) in older adults with a good safety profile.[17, 18]
Hyaluronic Acid (Oral): Clinical trials confirm efficacy for skin hydration, wrinkle reduction, and joint health.[19, 20]
Calcium Citrate: Prefer over carbonate for bioavailability; ensure total intake supports osteoporosis management without spiking arterial calcium.[21]
Tier 3: Experimental / Conditional (Re-evaluate)
Calcium Alpha-Ketoglutarate (Ca-AKG): Promising data on reducing biological age (epigenetic clock) and frailty, but lacks long-term hard outcome data.[22, 23]
Rapamycin: The gold standard for longevity in mice, but problematic for you. It raises lipids (counteracting Repatha) and interacts with Colchicine. Only consider if Colchicine is discontinued.[24, 25]
Tier 4: Low ROI / Deprioritize (Consider Dropping)
Blueprint “Essential” Stack: “Kitchen sink” formulation limits precision dosing. Contains B6, which carries neuropathy risks at high cumulative doses.[26, 25]
Methylene Blue: Failed to show consistent cognitive benefit in large AD trials; carries serotonin syndrome risk.[27, 28]
SS-31 (Elamipretide): While mechanistically interesting for mitochondria, it failed primary endpoints in clinical trials for heart failure and myopathy.[29, 30]
Low Dose Naltrexone (LDN): Evidence for dementia prevention is theoretical and weak compared to Lithium.[31]
Based on the critical interaction analysis and evidence hierarchy, the following items should be discontinued immediately or deprecated. The rationale is provided for each, prioritized by safety risk.
IMMEDIATE STOP: Rapamycin (Sirolimus)
Reason 1: Life-Threatening Drug Interaction: You are taking Colchicine for cardiovascular protection. Rapamycin is a potent inhibitor of P-glycoprotein (P-gp), the transporter enzyme responsible for clearing Colchicine from your body. Combining them can cause Colchicine to accumulate to toxic levels, leading to myopathy, rhabdomyolysis (muscle breakdown), and fatal multi-organ failure. This is a known, severe interaction.[1, 2, 3]
Reason 2: Lipid Conflict: Rapamycin increases LDL cholesterol and triglycerides by altering lipid metabolism.[4, 5] For someone with a CAC score of ~500 trying to crush Lp(a) with Repatha, taking a drug that actively raises lipids is counterproductive.
Verdict: Stop Rapamycin. Your cardiovascular risk is “here and now”; the longevity benefits of Rapamycin are theoretical and currently dangerous for you.
STOP: Methylene Blue
Reason 1: MAOI Interaction Risk: Methylene Blue acts as a Monoamine Oxidase Inhibitor (MAOI). While you are not currently listed on SSRIs, if you were to add one (or use certain pain meds/supplements like Tryptophan), the combination can trigger Serotonin Syndrome, a potentially fatal condition.
Reason 2: Failed Efficacy: Large-scale Phase 3 clinical trials (like those for LMTM, a derivative) have largely failed to show cognitive protection or reversal of Alzheimer’s pathology in humans, despite promising mouse data.[6]
Verdict: High safety risk, low proven reward.
STOP: SS-31 (Elamipretide)
Reason: Clinical Trial Failure. While mechanistically interesting for mitochondria, SS-31 failed to meet primary endpoints in significant human clinical trials for heart failure and primary mitochondrial myopathy.[7, 8] “Feeling it” is often a placebo effect in early peptide use.
Verdict: Expensive and currently unsupported by human efficacy data for your conditions.
STOP: Blueprint “Essential” Capsules
Reason 1: The “Kitchen Sink” Problem: You are taking this plus individual supplements (Lithium, Zinc, B-vitamins in other forms). This creates a risk of “stacking” doses. For example, uncontrolled B6 intake (pyridoxine) from multiple sources can lead to peripheral neuropathy.[9, 10]
Reason 2: Precision Dosing: As a high-complexity patient, you need to titrate specific variables (like Lithium for APOE4 or B12 for homocysteine) independently. A fixed-dose multivitamin prevents this.
Verdict: Switch to targeted supplementation for the few “essentials” you actually need (Methyl-B12/Folate if homocysteine is high, specific minerals) and drop the pre-mix.
Reason: Calcification Risk. You have a CAC score of ~500, indicating significant arterial calcification. While the data is mixed, several studies suggest that supplemental calcium (bolus dosing) may increase the risk of coronary artery calcification progression compared to dietary calcium.
Verdict: Obtain calcium from dietary sources (leafy greens, fortified foods) where absorption is regulated. If you must supplement for osteoporosis, use lower doses of Calcium Citrate spread throughout the day, but consult your cardiologist first.
STOP: Tremella
Reason: Vanity/Weak Evidence. The evidence for Tremella fuciformis is primarily limited to topical applications or animal models. Oral efficacy for skin quality in humans is not established compared to Hyaluronic Acid (which you are also taking and has better data).
Verdict: Redundant and likely ineffective orally.
Summary of “The Cut List”
| Item | Urgency | Primary Reason |
|—|—|—|
| Rapamycin | CRITICAL | Fatal interaction risk with Colchicine; worsens lipids. |
| Methylene Blue | High | Serotonin syndrome risk; failed Alzheimer’s trials. |
| SS-31 | Moderate | Failed human efficacy trials. |
| Blueprint Essentials | Moderate | Prevents precision dosing; toxicity risk from stacking. |
| Calcium Supplements | Moderate | Potential to worsen coronary calcification (CAC). |
| Tremella | Low | Low efficacy; waste of money/pill burden. |
Rapa 5mg weekly
Jardiance 25
Simvastatin 40/bemp acid 180/ezetimibe 10
Telmisartan 80
Acarbose 600
Retatrutide 4mg weekly (have to see interactions between acarbose/jardiance and want to move to retatrutide 10 weekly)
Dutasteride (let’s hope it minimizes the damage of male hormones)
Amitiza
Melatonin 40mg nightly (will get to 100 eventually)
Sirt 6 activator - donotage
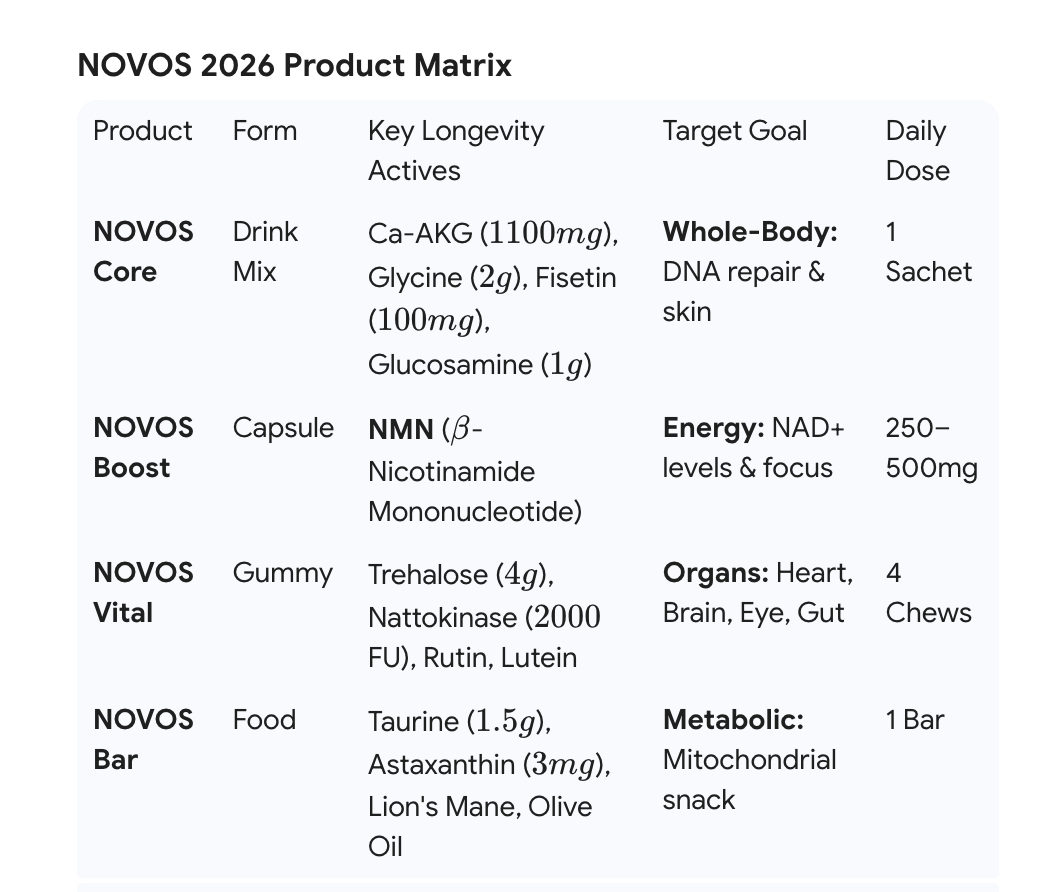
Novos core (is this worth taking still? Especially given monthly cost)
Magnesium/zinc/vitamin k2/A/D3 - all non synthetic
Glycine 15-20 grams daily
Psyllium husk
I want to do something with omegas cheaply after reading RapAdmin’s post but not sure what
Not wanting to be ripped off, I opted to have my own mix by looking at some of those high profile ones and the just buy quality brands and mix them up myself. FYI
Not sure anyone is expert enough to criticize your stack. But if you’re going to base it on science, then in my opinion, that means blinded, placebo controlled, prospective, repeated human studies. Very few supplements meet that criteria.
My stack has dwindled, and is clearly not proven benefit. There proof for some, personal positive experience for others, and some are n of 1 studies.
Metamucil
Creatine
TMG
Pectasol
Novos
Magnesium
Multivitamin
Fish oil
Vitamin d
Pendulum probiotic & polyphenol
Urolithin A
Sulforaphane
Blueprint longevity mix
Rapamycin currently 15 mg ageless rx compounded weekly (bought during the recent issues with shipments from overseas) I also just started back after a month break and trying less frequent dosing in 2025.
Rosuvastatin 5mg daily
Dapagliflozin 5mg daily
Ezetimibe 10mg daily
Dutasteride 0.5mg daily
Estradiol 75mcg patch semi-weekly
Testosterone cypionate 18mg sub-q weekly
Dhea 25mg daily (increased from 15 this week)
Boron 3mg daily
Lithium orotate 5mg 3 x weekly
Lugols iodine 1mg multiple days per week (when I remember-I live in the goiter belt). *notice nothing
Tretinoin topically 0.1% EOD
Vitamin D3 2k IU daily
*the last 2 are relatively new experiments for me over the last few months:
•White thyme or oregano essential oil (2 drops) in an enteric capsule with EVOO based on the Spice cabinet longevity article 5 mornings per week
•Trulacta 2 capsules nightly based a longevity book written by one of our fellow forum members.
As you’ve put all this info onto this site then I presume you are not paranoid about protecting this data?
What I’d suggest is that you use one of the AI apps, ChatGPT and Grok both work well from my experience, and put in all of the info you’ve shared along with a preamble on your bios. Then ask it to analysis and give you pros and cons for your medication, supplements, doses. You can also copy in bloodwork images and they will extract the dates and results so you’ll get a progressive view on your results. I’m not sure it can interpret your graphics but you could just use the core data and it should work.
Once you’ve done this you can integrate, correct and refine your queries and specific or new interests. You can ask advice on what to take together or split morning and evening, intermittent or regularly.
You can do the same with your daily skin routines and it will advise on the order you should apply various treatments to get the best responses. This is often based on the ph of the magic potions being applied. I did this for my wife who is a GP.
The data will all be kept in your chat history and you can return to update your regime or refine your queries. It’s not perfect but it’s totally logical and saves a lot of time in assessing where you are without copious notes all the long and complicated conversations.
Obviously, can print and share the outputs with your doctor or health advisor and it’s a great historical reference for when you started a new elements of your stack or regime.