neither does rapamycin, which only blocks mtorc1 but chronic mtorc1 inhibition leads to mtor2 inhibition, so it’s likely chronic meclizine use will lead to the same. Personally I would stick to rapamycin, which has only one target (mtorc1) unlike meclizine which has many different targets unless you have a hard time getting rapamycin
As I understood, rapamycin actually inhibits mTOR, which is part or both complexes, that is, its binding site is in fact with mTOR, and while this site stays accessible in mTORC1, it is not with mTORC2. Rapamycin will thus inhibit mTORC1 any time, and it will inhibit mTORC2 before its formation, if it can bind with mTOR. That’s why we must pulse it for antiaging purposes, to limit the inhibition of mTORC2 via the binding with mTOR (before formation of the complex 2). No?
4 Likes
There is a great deal to be learned about mTor inhibition with Meclizine., But, it is definitely an exciting new possibility that should be thoroughly explored. I looked on Ebay and see several sellers offer 1000 25mg tablets for under $40. Meclizine therefore is OTC and very economical. The possibilities should and will be tested. I am very interested in seeing what Dr. Richard Miller and the ITP report.
2 Likes
Is the fact that Meclizine, being an anticholinergic, may be bad longer term for brain health?
6 Likes
But if so, how can this be correct:
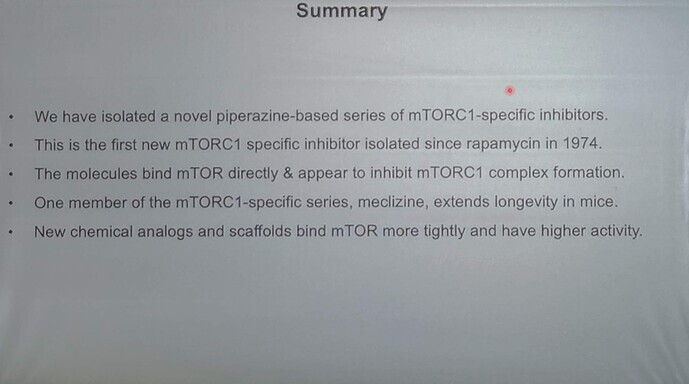
“The molecules bind mTOR directly” and “the first mTORC1 specific inhibitor since rapamycin”?
Either they bind mTOR and will inhibit all mTOR complexes, at least because they will have binded the mTOR that will be included in the complexes, or they bind mTORC1 only, and they are specific. ![]()
1 Like
My meclizine vs rapamycin experiment:
As I have posted earlier, I tend to sail with the wind. I am too old to do anything else.
At the halfway point of this year, it seems reasonable to me to switch from rapamycin to meclizine. After reading many papers I am looking forward to giving meclizine a trial run.
I will get my blood work done in ~ 3 weeks, ~30 days after my last rapamycin dose which was 15 mg taken with grapefruit juice. This will establish a personal baseline to measure the meclizine results against. The plan is to get my basic bloodwork done monthly.
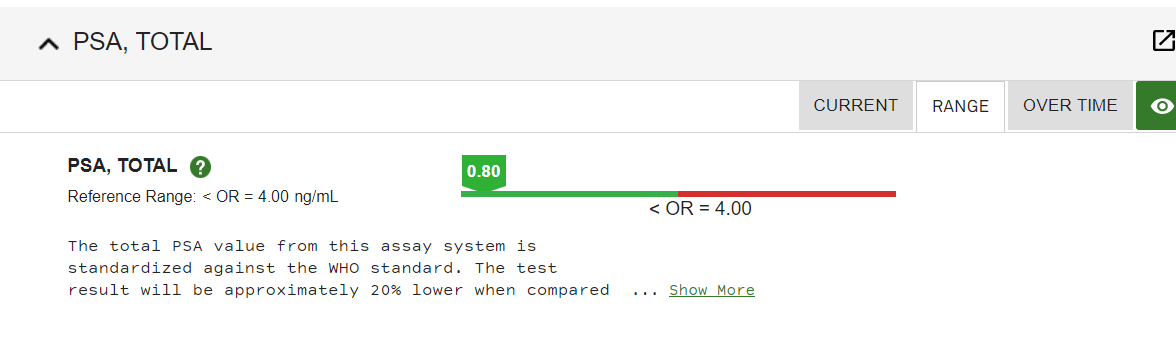
I will be taking meclizine at the 25 mg dose nightly. It was once part of my sleep stack so I am familiar with the possible side effects. It had no effect on my prostate that I am aware of. Meclizine didn’t have any effect on max urine flow. I have been taking tamsulosin for over 25 years and my PSA is 0.80 ng/mL
Meclizine seems to suppress mTORC1 without suppressing mTORC2. This is my main reason for switching at least temporarily.
The fact that meclizine is anticholinergic is not much of a worry to me as these first-generation anti-histamines are being purchased by the boatload by elderly people as part of their constant fight to get a good night’s sleep. The danger, while real, is also small.
To be frank, I have been a little underwhelmed by rapamycin, I don’t doubt its positive effects, but I was hoping for a little more subjective well-being and energy. Perhaps its negative effects on mTORC2 account for that fact, or, maybe I am just too old.
I am excited to be embarking on a new track for a while.
As you can see my doctor only orders this test every few years.
3 Likes
It’s an interesting experiment but I wouldn’t do it. This is especially true in the elderly.
Many drugs have an anticholinergic component and the list of side effects is significant, More than rapamycin actually ,and I’ll frankly be shocked if you feel younger with it, but who knows.
Also, if you’re suppressing mTOR daily, isn’t that similar to what renal transplant patients do?
1 Like
The difference as I understand it, daily use of rapamycin also suppresses mTORC2. As I said, I have taken meclizine daily, in the evening, in the fairly recent past for 60 days or so, and experienced no adverse effects. I wasn’t aware at the time that it was an mTORC1 suppressor. I will be keeping a close eye on things.
2 Likes
I guess I’m wondering if it’s safe to inhibit TOR 1 on a daily basis.
1 Like
FWIW
Klickstein states there should be a break.
Review Attia interview;
#118 – Lloyd Klickstein, M.D., Ph.D.: Rapamycin, mTOR inhibition, and the biology of aging
1 Like
We certainly don’t know the long-term safety effects of rapamycin either.
I can’t find any long-term safety studies for meclizine, but it has been around for a long time and I don’t see any particular warning flags other than the anticholinergic effect.
I also think mTORC1 suppression is dose-dependent with meclizine, as it is with rapamycin.
The 25 mg. daily dose of meclizine is at the low end of dosages used in studies.
Because I was already in pretty good shape from using keto and time-restricted feeding, both of which lower mTORC1, my Levine spreadsheet biomarkers were not improved by the use of rapamycin for 8 months.
Only my HDL improved, and that is a questionable marker. Meanwhile, my lipid panel certainly took a turn for the worse.
Two other adverse effects I noted were delayed wound healing, especially if happened right after a dose of rapamycin, and the thinning of my fingernails.
“side effects associated with long-term rapamycin treatment, many of which are due to inhibition of a second mTOR complex, mTORC2, have seemed to preclude the routine use of rapamycin as a therapy for age-related diseases.”
In any case, I will keep a close eye on my physical and mental health while taking meclizine.
“A study evaluated the memory effects of meclizine 25 mg, lorazepam 1 mg, promethazine 25 mg”
“The authors found that meclizine produced the least amount of detrimental memory effects in that it did not significantly decrease overall accuracy of answer choices or increase the time to make a choice,”
“Since 1962, there have been several trials demonstrating meclizine’s safety in pregnancy.29,30 One study evaluated a total of 50,282 mother-child pairs.30 Of these, 1,014 mothers had taken meclizine during the first four months of pregnancy. The rate of all malformations combined among those not exposed to meclizine was similar to that in the exposed group”
Meclizine: Safety and Efficacy in the Treatment and Prevention of Motion Sickness
https://journals.sagepub.com/doi/full/10.4137/CMT.S6237
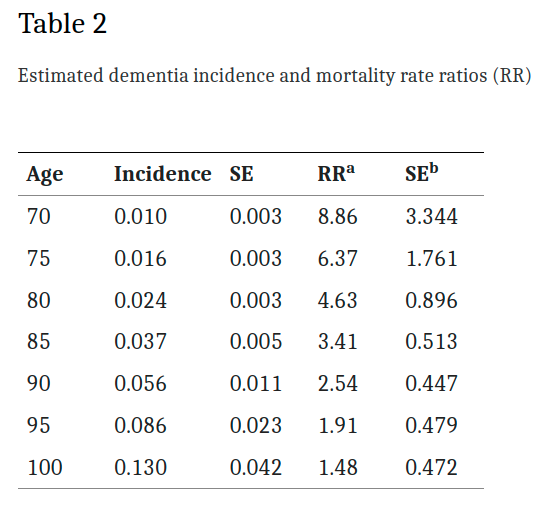
“Moderate Inhibition of mTORC1 Signaling is Sufficient to Extend Lifespan and Healthspan
Fascinatingly, short-term late-life rapamycin treatment is sufficient to extend longevity”
“side effects associated with long-term rapamycin treatment, many of which are due to inhibition of a second mTOR complex, mTORC2, have seemed to preclude the routine use of rapamycin as a therapy for age-related diseases.”
3 Likes
I stand to be corrected, but I thought fingernails/toenails constantly thickened with age, therefore the thinning of such might be a sign of turning the clock back???
1 Like
I would do a washout period, though. It will be interesting to see whether your lipids then improve, how much and how fast. If they improve well and fast, it might indicate that you dosed rapamycin too aggressively.
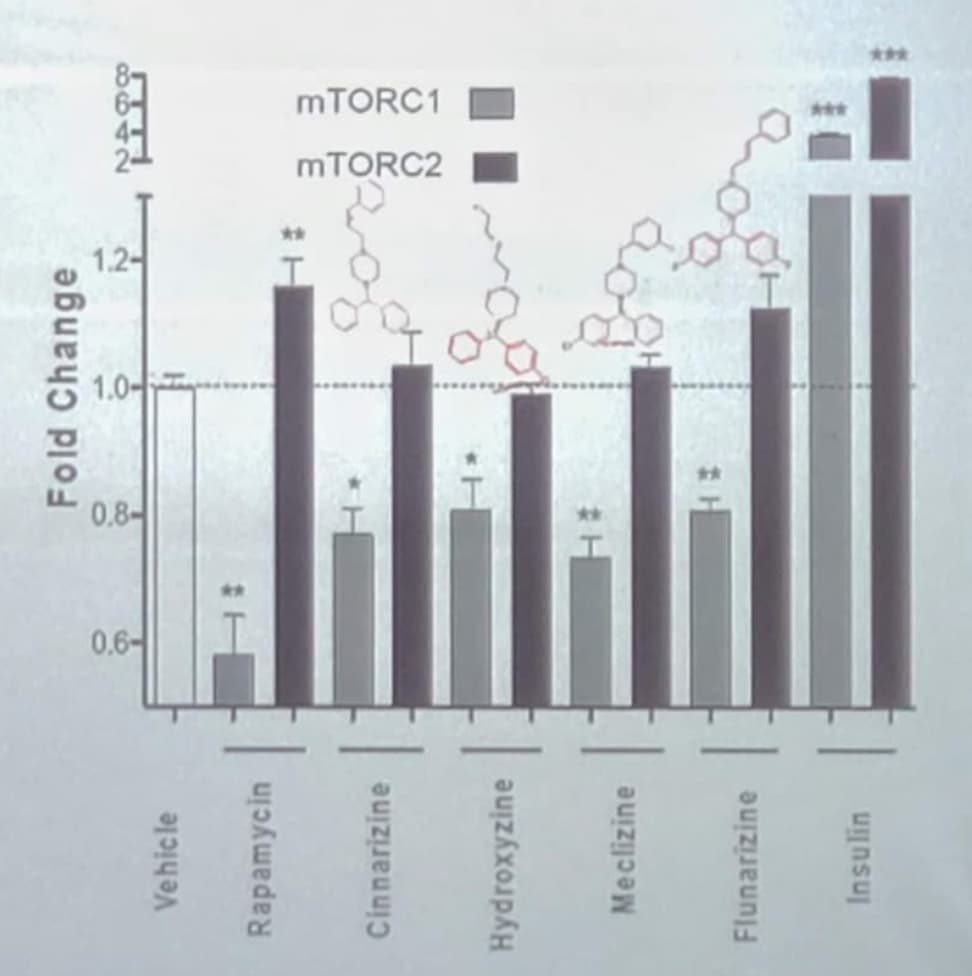
And I have to say I’m still skeptical about that “specific mTORC1 inhibitor”. Actually, when you look at the results on the slide above (that I copy below), it looks like C1 is less inhibited by this new candidate than by rapamycin, while C2 is more inhibited. But perhaps I don’t read it correctly?
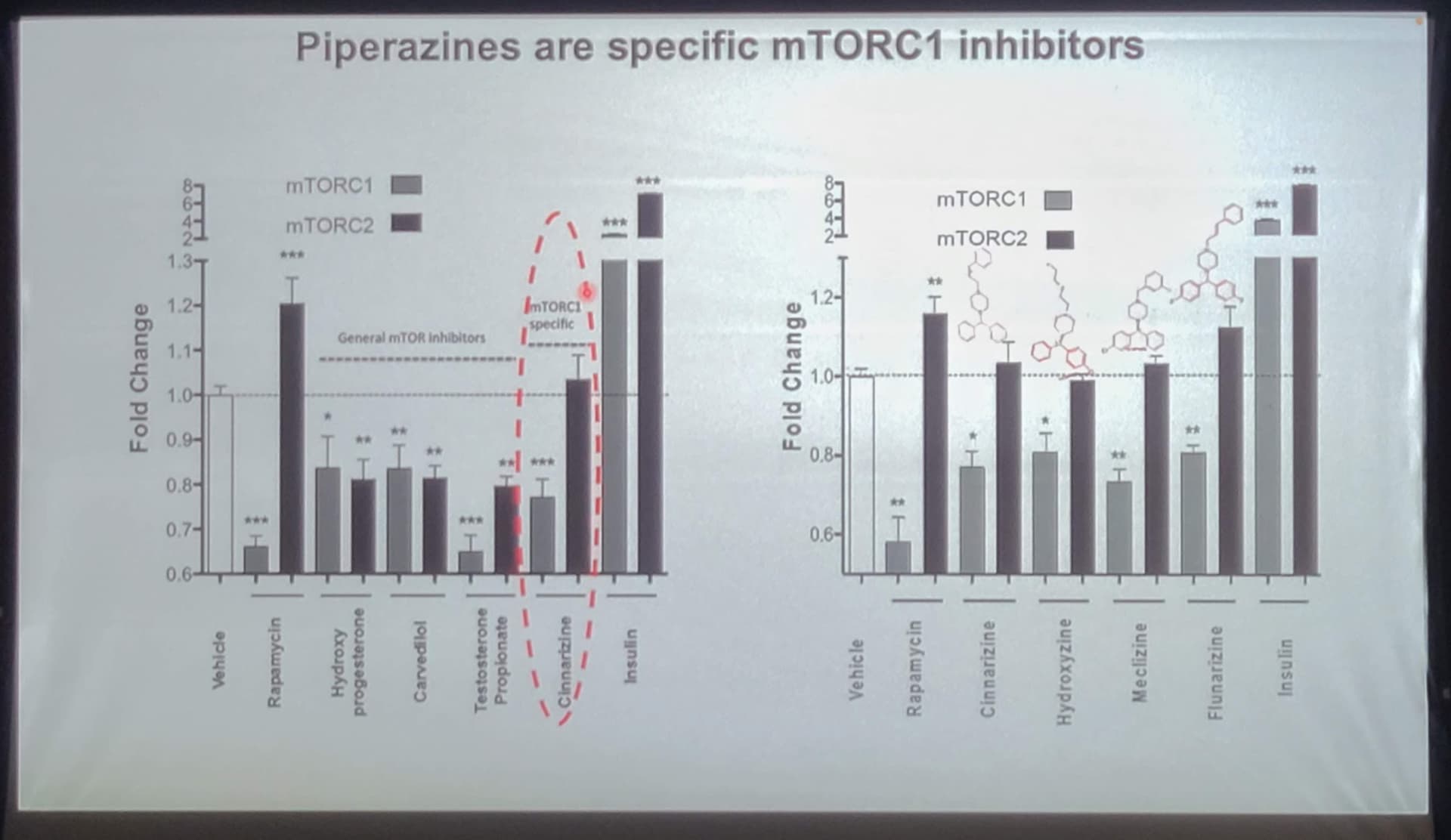
The only clearly positive point of those slides (to my eyes) is the extended lifespan in mice.
2 Likes
Yes - that is true. In this study, Meclizine was not as good an mTORC1 inhibitor as was rapamycin, but the reason they are looking at all these drugs is that they would like to find a drug with similar (or at least close) mTORC1 inhibition, but no mTORC2 inhibition (and therefore, the theory goes, fewer negative side effects such as immune suppression at high doses).
In the above slide (I’ve pulled out the one graph to focus on below) you can see that Meclizine is the best of this bunch (other than rapamycin) at inhibiting mTORC1, with minimal effect on mTORC2. An interesting question that was brought up earlier in this discussion is whether mTORC2 inhibition naturally starts happening over time any time you start inhibiting mTORC1 for longer periods of time? This is a good question - we’ll need to ask the researchers about this issue.
An Additional note - the other drugs listed here all do a pretty good job (other than Insulin, obviously, which I think was just included for comparison to something that obviously has a pro-aging effect with the IGF-1 connection). So the drugs:
- Cinnarizine
- Hydroxyzine
- Flunarizine
Would all seem to be good potential anti-aging drugs also. I suspect that all of them likely increase lifespan if they were tested in mice. If someone has the time - perhaps they can look into these mTORC1 inhibitors also - and see if any of them have obviously better side effect profiles.
2 Likes
We need to look more into this - its an area I have not explored. It seems there is a scale of anticholinergic drugs, and since Meclizine is not listed as one of the typical anticholinergic drugs, I wonder how anticholinergic it is relative to the other drugs on that list.
I do see this when I look up anticholinergic drugs:
Conflicting conditions
Anticholinergics can be used to treat many conditions, but they aren’t for everyone. For example, these drugs aren’t usually prescribed for older people.
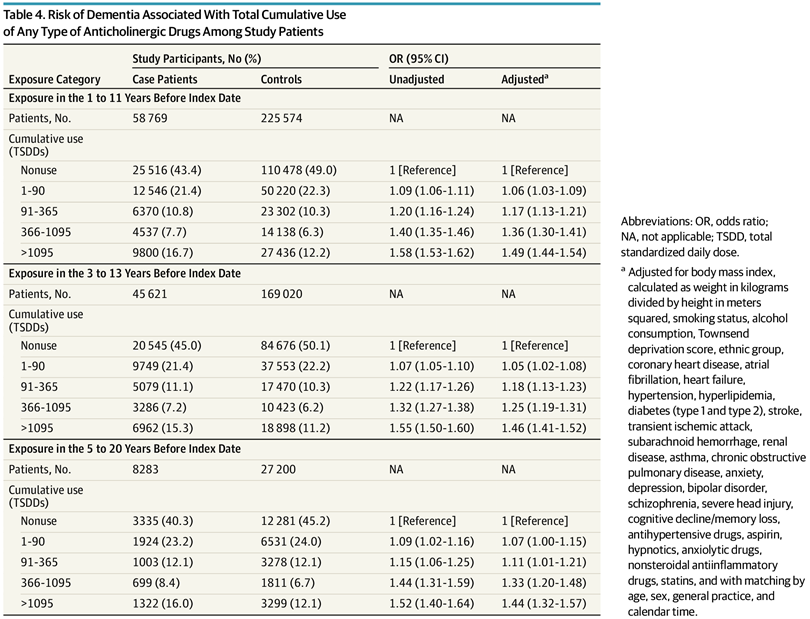
Anticholinergics are known to cause confusion, memory loss, and worsening mental function in people who are older than 65 years. In fact, recent studiesTrusted Source have linked use of anticholinergics with increased risk of dementia.
Also, people with the following conditions shouldn’t use anticholinergics:
- myasthenia gravis
- hyperthyroidism
- glaucoma
- enlarged prostate
- hypertension (high blood pressure)
- urinary tract blockage
- increased heart rate (tachycardia)
- heart failure
- severe dry mouth
- hiatal hernia
- severe constipation
- liver disease
- Down syndrome
This research paper below is cited in the above reference on Healthline.com:
Anticholinergic drugs and dementia in older adults
gray2018.pdf (631.8 KB)
1 Like
There are certainly some pros and cons.
Pros:
- Might well be more TOR 1 specific.
- Antihistamines have been in use forever. Generally well tolerated.
- Doubt that glucose or lipids will be much affected.
Cons:
- Meclizine is usually dosed short term for motion sickness and vertigo. Not long term.
- Still guessing about dosing.
- Is chronic TOR 1 inhibition a good idea and will it lead to TOR 2 inhibition over time.
- Long term interference with acetylcholine activity can be an issue, especially when combined with other meds that have some anticholinergic actions.
2 Likes
Not unless you’re talking baby. My fingernails became very thin and tear easily.
More on this topic of anticholinergic drugs and brain impact. It seems that Meclizine is a pretty strong anticholinergic, and is high on the anticholinergic cognitive burden scale. See below.
In 2008, Indiana University School of Medicine geriatrician Malaz Boustani developed the anticholinergic cognitive burden scale, which ranks these drugs according to the severity of their effects on the mind. It’s a good idea to steer clear of the drugs with high ACB scores, meaning those with scores of 3. There are so many alternatives to these drugs.
NOTE: Meclizine has a score of 3, on the cognitive burden scale as shown below. (So this is not looking good in that respect)
Source: Harvard Health
Anticholinergic-cognitive-burden-scale.pdf (309.4 KB)
2 Likes