This is an idea which has been formualted by David Sabatini in his epic podcst with Matt Keiberlein and Peter Attia. In a few words, he told that he was thinking about inhibiting m-TOR by acting upon the upstream signals. He told no more. We had a discussion on this which I could not find, but I’ve been occasionally mulling over this topic. Then, when I heard that the recent Gemini 3.1 Pro may have reasoning capabilities similar to the alpha-fold model. So I decided to ask to him (anthropomorphized).
Q: Consider all the evidence we know on the mTOR biological system, especially so the upstream signals which can activate the mTOR complex systemically or inhibit it. Now select the following which can act on the upstream signals and inhibit mTOR in a fashion similar to rapamycin: 1)specific diet and foods, 2) specific physical activity; 3)specific supplements; 4) specific sleep habits. 4) other non pharmaceutical interventions. Also specify theestimated degree of inhibition.
The answer has been very extensive and went beyond what I originally wanted. Since it is not a short one, I am attaching the PDF. I did not pirsue the loogarithmic model since the server blocked, probably because of the limitations to my free acount.
This is the answer from Grok 4.20 beta model. less quantitative, perhaps more actionable in the details, even a menu was provided. Overlapping to Gemini’s answer in many aspects.
The m-TOR optimization plan is optimized to my phenotype and age and habits. It can be adjusted to anyone of course.
I cannot presently use Rapamycin because of unavailability, lack of risk-appetite, lack of close monitoring possibilities, and uncertain risk-to-benefit ratio.
Sorry, you cannot use rapamycin. I read the paper and did not find the alternatives very appealling. I am placing my bet on weekly rapamycin pulse dosing.
Yes - I think @mccoy just made a strong argument for the use of rapamycin. You have two options… do this long list of actions, some of which are very difficult (strict calorie restriction), or take this single drug. Most people would prefer to simply take the drug (rapamycin) - easy, quick, effective.
We all unquestionably agree that that’s the fastest, no-fuss way to act on mTOR.
On the other side, beyond having access to rapa, it takes close monitoring of blood concentrations if we want to do that rigorously and to prevent unwanted side effects.
Also, its usefulness for healthy individuals below 70, may be sometimes arguable. Surely, Joan Mannick advises against it for under-70s
And last but not least, we don’t have yet any conclusive evidence from trials. Sorry for playing the party-pooper but we all know well pros and cons.
In a few years I may be taking it or some better analogue, or hopefully be taking something else discovered after the application of the Isomorphic Labs project.
With that many molecules on a specific timetable you end up with a very fragile chain with multiple points of failure. I’m not a fan. A ton of this is arbitrary, contradictory and unknowable. Telmisartan “in the morning”, but also 24 hour half-life, either/or. Why “morning” if 24 hour? The more molecules you involve, the greater chance of unexpected and unanticipated interactions not just within the stack, but outside the stack (food, other drugs and supplements, exercise and other lifestyle factors). Many of these are poorly supported by evidence (like fisetin among others), or need very specific conditions to be effective (like quercetin), are very dirty (like curcumin among others). Odds that this stack will work in perfect concert to achieve the desired results - extremely low. Very poor ROI in required effort to possible results.
There’s a reason why a single molecule like rapamycin has higher (though ultimately unknown in humans) odds of successful outcomes than attempting to get there through a complicated rube goldberg stack of dubious supplements.
I don’t think the squeeze is worth the juice in this case with this stack. Of course, YMMV.
Possibly true and I always wonder what the border between diet and supplement diversity looks like. I’m also inclined to think about supplement stacks as compounding error terms but future findings will no doubt illuminate this area further, perhaps even showing this thinking to be an artifact dragged over and misapplied from our training in statistics. Then there is the challenge of isolating independent variables in order to assess effects. This is comparatively easy with a single compound pharmaceutical and at times impossibly difficult when examining diets or supplement stacks.
Beyond that, some who are interested in geroprotection cannot or choose not to take rapamycin (or some other drug). Given that we early adopters are generally risk tolerant experimentalists operating years in front of confirmatory data, experimentation with stacks seems like one fruitful avenue. Why not.
I really cannot, since there is no availability here; if mailed from India it would be held at customs as an illegal import
Even if I could, actually I would still be reluctant presently, for various reasons (my age, my state of health and my degree of belief).
The use of rapamacyn as a gerosuppressant is still not supported by evidence, but by degrees of belief, which is fine nevertheless. We very often navigate by degrees of belief.
Here is Italy, Europe. The only way to have Rapa would be to go fetch it with some difficulties in Turkey or Dubai (not advisable right now!!). Those are the closest places. Of course I may go to Mumbai or Dheli.
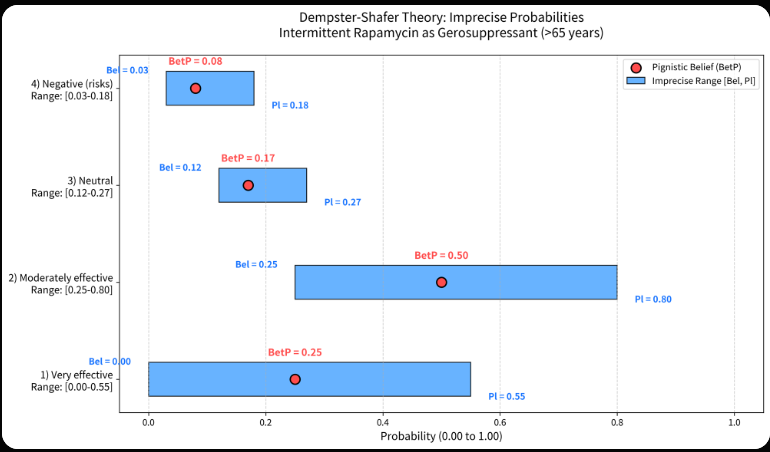
But, since I mentioned degrees of belief, I wanted to go deeper and proposed an interesting question to Grok 4.2 with its new quadruple agents architecture. They work in parallel and debate, fact-check, and collaborate to improve accuracy and reduce hallucinations.
I asked to collect all relevant info in the web and provide the degrees of belief by the DS theory of 4 scenarios, for the intermittent use of rapa by > 65 yrs individuals.
the result is, again, interesting. As expectable, the ranges of probabilities are very wide.
I’m attaching the PDF and the shareable link to the question. thanks to mod, his suggestions have been useful to eliminte the annoying characters.
PLEASE NOTE that the first plot is wrong, ranges are not aligned, the following one is the right one.
I would think that Rapa is a prescription medicine in Italy where some medics will prescribe it. If you disagree with this I will do some searching for evidence.
Absolutely. And you have just indicated one of the big reasons why I prefer pharma drugs vs most supplements. One big reason is that drugs are extensively tested in a variety of people with a variety of diet, lifestyle and polypharmacy profiles. And we have clinical experience - often for decades. If the drug works despite all that variety, that tells me that this particular molecule can be “trusted” to at least be somewhat effective without fears that diet and other factors might cause unexpected interactions. This by the way, was one of the considerations frequently mentioned on the CR list (RIP) - when discussing supplements or drugs, there was the common lament that unfortunately the CR diet is so extreme that odds are any given supplement or drug studies in ad lib cohorts have limited applicability to the CRON crowd. In other words, even with pharma drugs there still are caveats around extreme diet, exercise or lifestyle factors (ahem, biohackers).
Still, databases around pharma drugs are so extensive that it’s easier to track interactions, especially that you are dealing with known dosages and formulations. But supplements are a whole other ball game. Hence, again, I think a single pharma drug, like rapa, even though it’s being used waaaay off label by LE enthusiasts, is still a “safer” bet (even though still very speculative) than trying to replicate that effect through a bunch of supplements.
Having said all that, I agree - we are risk tolerant (to various degrees) and willing to experiment. I’d be the last person to criticize polypharmacy. Still, I prefer to start with pharma drugs. As an example, since telmisartan was mentioned, I take 80mg telmi and I also take 25mg empagliflozin. I shamelessly speculate mechanistically that the interaction will be largely synergistic for renal health and possibly in other contexts (endothelial tissue). Do I know that for a fact? Only studies of both used at the same time can show that*. But I’m grateful for the amount of data available on those two drugs. That’s not true for most supplements, and so my gamble there is orders of magnitude more uncertain with supplements.
Experiment away, but if not necessary, why take risks. In my mind, rapamycin (if tolerated and practical) is the better bet in this case compared to that stack. YMMV.
*Example of a study of both, unfortunately from India (giant cautionary alert!):
Assessing Renoprotective Effects of Empagliflozin and Telmisartan Combination Therapy in Non-albuminuric Diabetic Nephropathy: A Retrospective Cohort Study
We need to check the bathwater. There is abundant evidence of synergy among foods and among 2, 3, and even 4-way supplement stacks, likely more so than with pharma, as evolutionary biology might predict. A messy IV/DV matrix for sure but not an empty construct.
The clarity of a causal path is independent of its significance.