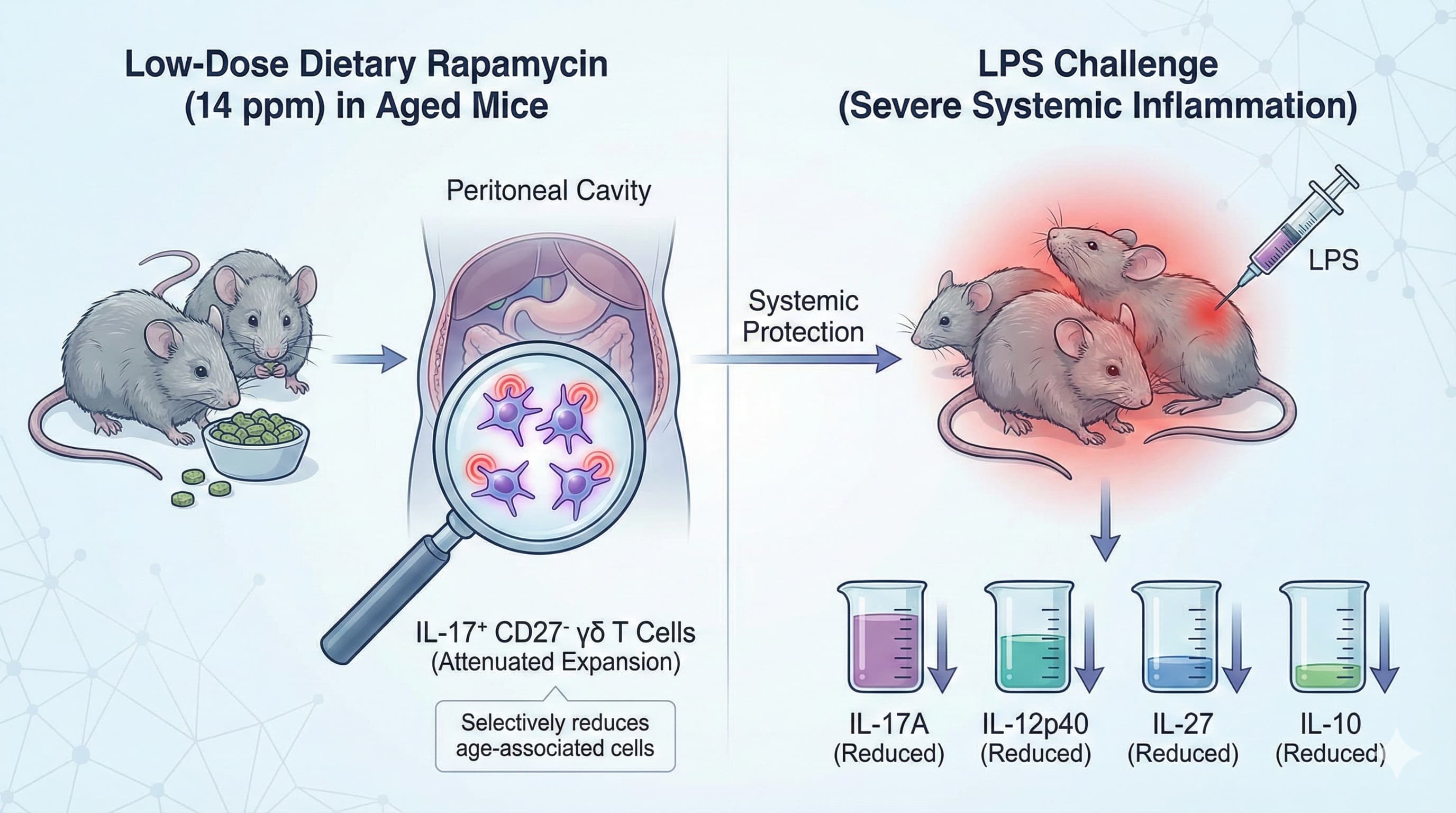
Aging drives progressive immune remodeling and chronic basal inflammation, a phenomenon known as inflammaging. While inhibiting the mTORC1 pathway with rapamycin is known to increase lifespan across various species , its long-term clinical utility as an anti-aging intervention is frequently debated due to concerns regarding broad immunosuppression. This preclinical study demonstrates that prolonged, low-dose dietary rapamycin administration (14 ppm) in aged mice does not induce systemic immune suppression or significantly alter circulating myeloid and B cell populations.
Instead, the intervention selectively attenuates the age-associated expansion of IL-17-producing CD27- γδ T cells, specifically within the peritoneal cavity. Furthermore, when subjected to a severe systemic inflammatory challenge via lipopolysaccharide (LPS), aged mice treated with rapamycin exhibited significantly reduced circulating levels of IL-17A, IL-12p40, IL-27, and IL-10. This blunting of peripheral cytokines correlated with an attenuation of neuroinflammation, marked by reduced expression of reactive microglial genes, including Tnf-a, Il6, and Tlr2. The primary conclusion is that continuous, low-dose rapamycin acts as an immune recalibrator rather than a non-specific immunosuppressant, targeting distinct inflammatory nodes to preserve central nervous system homeostasis in older subjects.
Source:
- Open Access Paper: Long-term rapamycin treatment suppresses IL-17-producing gamma delta T cells and blunts neuroinflammation in aging
- Institutions: The research was conducted collaboratively by the German Center for Neurodegenerative Diseases (DZNE) in Germany, the Barts Cancer Institute at Queen Mary University of London in the United Kingdom, and University College Cork in Ireland. It is currently published as a preprint in bioRxiv.
- Impact Evaluation: The impact score of this journal is 0 (Preprint server),