Read Preston Estep’s Mindspan - it syas A LOT about canola oil (and is also pro-canola oil)
Your two staples when it comes to cooking should be olive oil and canola oil,[*](javascript:void(0)) both of which have high MUFA content, and canola has a good balance of omega-3 and omega-6. Try to use less soya bean oil, and minimize “vegetable” oils such as corn, common safflower, and sunflower, which all have much higher levels of omega-6 EFAs. Here are some other tips:
• Buy cold-pressed canola oil, which has been pressed to release its oil and processed at lower temperatures. Many supermarket varieties of canola oil are not cold-pressed but instead are hydrogenated to prevent the PUFAs from oxidizing.
• Always store canola, soya bean, and flaxseed oils and walnuts, pecans, and other high-omega nuts in a sealed airtight container, preferably in the refrigerator. This will help prevent oxidation.
CANOLA OIL. Canola oil is the primary oil in the Japanese diet. I follow their example and use canola oil for low-temperature sautéing and a variety of other uses, including some salad dressings. Always purchase cold-pressed canola oil in amounts you can use in two months or less, and keep it in the refrigerator.
There’s a difference between expelled-pressed and hot-pressed, which is important, but not as important as it is for more polyunsaturated fats. Beyond Meat uses canola oil and uses a kind of processing that doesn’t heat the oil as much as it does for standard canola oil (though still not the best extraction process)
Canola oil is more MUFA than PUFA and rapeseed has a surprisingly high content of polyphenols/antioxidants.
Rapeseed oil is characterized by the ideal polyunsaturated fatty acid content with a 2:1 ratio of linoleic (n-6) versus
linolenic (n-3) fatty acid and high contents of active biological
compounds, such as tocopherols, plastochromanol-8, phytosterols and
phenol compounds [12–15].
Rapeseed has the highest phenolic content among to other oilseeds
(soybean, sunflower), about tenfold, however, phenols remain in the meal
after pressing [16]. Phenol compounds, including sinapinic acid and other derivatives, show high antioxidant activity under in vitro conditions [17].The
main phenol compound of rapeseed is sinapinic acid, which makes up 70%
of the total content of free phenolic acids and their derivatives such
as sinapine [18]. Other derivatives of sinapinic acid that have been identified include 1-O-β-d-glucopyranosyl sinapate; 1,6-di-O-sinapoylglucose; 1,2,6′-tri-O-sinapoylgentiobiose;
sinapic acid methyl ester, 3-dihexoside-7-sinapoyl-hexoside kaempferol
and 3-hexoside-7-sinapoyl hexoside kaempferol [19–23].
During rapeseed roasting and pressing, a sinapinic acid decarboxylation
product is formed and transferred to the oil producing an oil enriched
with high antioxidant activity compounds [24, 25].
In the literature, data are available on the effect of roasting and
microwaving of rapeseed and mustard seeds on the content of native
bioactive compounds including canolol [26–30].
However,
these studies are concerned with black rapeseed. There is no data on
the effect of the roasting process on yellow-seeded rapeseeds, which are
characterized by thinner seed coats and lower fiber contents.
The bioactive constituents of canola oil are phenolic compounds, tocopherols, phytosterols, and carotenoids [47].
The phenolic compounds in CNO are mainly phenolic acids: sinapic acid,
cinnamic acid, syringic acid, ferulic acid, 4-hydroxybenzoic acid,
vanillic acid, and p-coumaric acid [49].
The heat treatment prior to rapeseed cold-pressing for the CNO
obtaining process induces sinapic acid decarboxylation, resulting in
canolol [50];
an oil-soluble bioactive phenolic compound that is easier to extract
into CNO. It has significant antioxidant, antimutagenic, and
anticarcinogenic effects [51].
Tocopherols of canola oil are γ-tocopherol and α-tocopherol, as the
major tocopherols, while δ-tocopherol, plastochromanol-8 (PC-8), and
β-tocopherol are the minor tocopherols [51].
The main CNO phytosterols are cholesterol, brassicasterol (specific for
rapeseed oil), stigmasterol, campesterol, β-sitosterol, and Δ5
-avenasterol [51]. Finally, β-carotene, zeaxanthin, and lutein are the CNO carotenoids [46]. The hydroxyl group (–OH) of phenolic compounds, tocopherols, and phytosterols can scavenge the free radicals [47], with CNO being known for its considerable antioxidant properties.
CO consumption significantly reduced TC (-7.24 mg/dl, 95% CI, -12.1 to
-2.7), and LDL (-6.4 mg/dl, 95% CI, -10.8 to -2), although it had no
effects on HDL, TG, Apo B, and Apo A1. Effects of CO on TC and LDL
significantly decreased after CO consumption in subgroups of >50
years of age participants and >30 intervention duration subgroup.
Moreover, CO decreased LDL and TC compared to sunflower oil and
saturated fat
Yes the data and evidence suggest it is the healthiest fat source. It is the lowest amount of SFA in it compared to all other fat sources, and it lowers LDL, TG etc more in comparison to olive oil:
So it is a concentrated source of PUFAS with very low SFA and lowers LDL, TG etc better than olive oil which isn’t suprising since olive oil has more MUFAs and low PUFAS which lowers LDL etc less, and twice the amount of SFA per 100 g.
That study could be confounded by trans fats and trial participants could enter or leave the study whenever they wanted which is problematic for the internal validity.
See section Heart Disease, or search for the trial here:
Most talking head doctors are motivated by money and attention I think. The best way to get that is to tell people what they want to hear. Supply and demand.
LDL is very correlated with apoB, TG a little so too.
I can’t find how many left need to dig deeper but most of these people probably weren’t in these institutions on their own accord.
Incidently I did find that they specifically used unhardened margerine and soft corn oil as substitutions
Edit:
Of the 2403 pre randomisation records that were retrieved 2355 had a post randomisation record, so only 2% drop out (and around 7000 records lost)
I have a question. I don’t use seed oils for anything other than just spraying it (canola oil) on my cast iron pan to keep meat from sticking to it. I use canola oil because it is essentially tasteless.
So assuming canola is bad, do you think this amount is harmful?
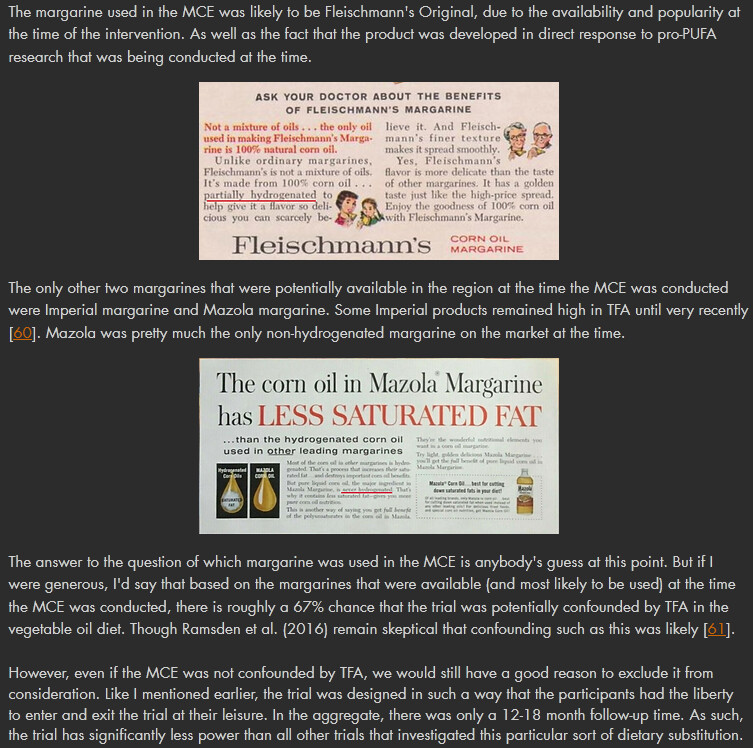
What specific oils and margarin? In the ad you can see the Fleischmann’s Original is partially hydrogenated. Nowhere does it say they excluded partially hydrogenated oils or margarine.
They used to use rapeseed (canola) oil as oil for painting because it sets (forms cross linking chemical bonds) I think once it sets it should be fine. Omega 6 oils are even essential but we get way too much of those and too little omega 3
So both diets contained equal amounts of transfats
Control diet
The control MCE diet was patterned after the “D” diet of the National Diet Heart Study. It was designed to appear similar to the experimental diet. Notably, free surplus USDA food commodities including common margarines and shortenings were key components of the control diet, making the daily per participant allocation from the state of Minnesota adequate to cover the full costs.21516 As common margarines and shortenings of this period were rich sources of industrially produced trans fatty acids,232425 the control diet contained substantial quantities of trans fat. Compared with the pre-randomization hospital diet, the control diet did not change saturated fat intake but did substantially increase linoleic acid intake (by about 38%, from 3.4% to 4.7% of calories). Based on this increase in dietary linoleic acid alone, the Keys equation predicts that the control diet would lower average serum cholesterol compared with baseline (fig 3⇑ and table 2⇑). This reduction, however, would be modest compared with the reduction in the intervention group.
Nowhere does it say they contained an equal amounts of trans fats. Increasing margarine (“soft margarine”) intake when most of the margarine at the time had high levels of trans fats means it’s likely that trans fats increased by a lot.