FASCINATING! Thank god I’m not a fly.
So I’ve got massive Sirolimus, my lipids and glucose are CLASSIC mTOR markers, gut microbiome alteration, anemic, but yet I’ve got no MTOR inhibition? I don’t believe it.
FASCINATING! Thank god I’m not a fly.
So I’ve got massive Sirolimus, my lipids and glucose are CLASSIC mTOR markers, gut microbiome alteration, anemic, but yet I’ve got no MTOR inhibition? I don’t believe it.
There are a plethora of rapamycin/mice studies use DSMO as the vehicle.
https://sci-hub.se/http://dx.doi.org/10.1136/annrheumdis-2011-200557
“Rapamycin was obtained from LC Laboratories (Woburn, Massachusetts, USA), dissolved in dimethyl sulphoxide (DMSO) at 25 mg/ml and stored at −20°C. For injection, the stock solution was diluted in phosphate buffered saline (PBS). Mice received daily intraperitoneal injections of rapamycin at 1 mg/kg body weight/dose in a total injection volume of 0.3 ml for 10 weeks and control animals received the DMSO vehicle at 0.4% in a total injection volume of 0.3 ml”
Some additional interesting properties of DSMO as my carrier.
It’s a natural antiseptic.
https://onlinelibrary.wiley.com/doi/10.1002/jps.2600580708
And here’s another magical property of DSMO…perhaps of huge benefit getting Rapamycin thoroughly inside body tissue, something far more difficult with plain oral delivery?
“In the body, DMSO can pass through cell membranes as readily as water does without damaging the tissues, and it can replace water molecules within many bodily fluids. And, because DMSO so readily dissolves other molecules, it can also carry them through the cell membranes with it. “DMSO alters cell membrane permeability,” says Jacob. “It moves through membranes and substitutes for water so that it pulls substances through cells that ordinarily would not move through them. This is its basic mechanism of action.”
This is all new unexplored frontiers…
I am sticking to my 2mg pharmacy issued sirolimus pills and grapefruit juice. Lol
Yeah well I’m trying to increase my odds and make this a fair fight!
You even have “glowing” hair now…geez.
As post back on April 7, 2022
uploaded a PDF copy of
“Dimethyl Sulfoxide (DMSO) in Trauma and Disease” by Stanley W. Jacob and
Jack C. de la Torre
The book on DMSO
Selected Contents
Chemistry of DMSO. DMSO in Basic Pharmacology. DMSO Clinical Pharmacology.
DMSO in Genetics. DMSO in Basic Microbiology. DMSO in Clinical Microbiology.
DMSO in Malignancy. DMSO in Basic Neuroprotection. DMSO in Clinical
Neuroprotection
You know - I might give Fabio a run for his money on this hair thing. My hair is getting real “purty”, soft and silky. Amazingly rich in color and shine. LOL.
No joking, you guys are the same age too…doppelgängers (well, getting there).
But he’s got one up on you…a skin care line, but not hair. What are you waiting for??
In 2021, he launched a hair and skincare line for men titled Aston James, with the help of two Australian entrepreneurs
So I had my first post IM+IN rapamycin doc consult yesterday.
On lipids, of course, some concern…but he’s deferring to my upcoming cardiologist consult.
On the anemia, surprisingly sanguine. He figures with my chronic blood donations, my body has adapted to the low iron now (re not being symptomatic or athletic diminution). He use to consternate before I blew by his red line “not < 80 ferritin” a long time ago. TRT also stimulates red blood cell production, so perhaps an underlying resiliency buffer. Could also be partly my iron genes.
On the rapamycin, I had to explain the markers rise was entirely from the recent intervention, including the PSA (he didn’t know what to make of the blip either). Also deferring to my urologist, once I have more duration/transiency data. He knew I started experimenting with rapamycin last year. He knows a little about rapamycin (thank god for Attia…doc says if Attia’s taking it, it must be ok!). His biggest concern is immunosuppression, so he’s adding a deep biomarker panel to capture. As well, more short term markers followup tracking testing (1 month, 3 month) including more sirolimus levels. He didn’t even chastise me for the IM+IN vs oral.
On the whole, extremely supportive of my journey.
Actually I am 1 year older. Born April 1958…
He’s looking good… for his age… hahaha.
With all the junk he’s had slathered in that voluminous hair (and absorbed systemically) over the decades…no way his biological age is lower than yours.
Definitely. Lol.
I am impressed with your physician’s support.
Sounds rare from the members on this site.
Glad my Physician sees his role is to guide… not dictate… and try reasonable treatments and supplements. Rapamycin, TRT, oral Minoxidol, Metformin. All reasonable.
My transformation can’t be denied…so he is more flexible than ever.
@MAC - You may have answered this already, but did you consider subcutaneous injections over IM? I am sure you have good reasons.
Not too deep, the normal reasons:
“The speed of absorption is faster for intramuscular injection compared to subcutaneous injection. This is because the muscle tissue has a greater blood supply than the area just under the skin. Muscle tissue may also hold a larger volume of medication than subcutaneous tissue.”
“Sirolimus is a highly lipophilic compound with a high blood to plasma ratio and small free fraction in plasma. In general, the adipose tissue is a storage compartment for lipophilic compounds with slow release from this storage site resulting in long elimination half-lives.”
So I didn’t want rapamycin lingering in fat tissue, and thus bioavailability and AUC is generally lower for SC vs IM.
https://www.nature.com/articles/s41565-021-01048-2
“These results demonstrate the ability of engineered nanocarriers to repurpose drugs (rapamycin) for alternate routes of administration by rationally controlling cellular biodistribution”
The above SC delivery route paper showed that SC was a more targeted approach whereas I wanted wide pan tissue volume of distribution.
The same paper also showed quite fundamentally the huge benefits (reduced side effects) of bypassing oral delivery:
“These results demonstrate the ability of a rationally designed nanocarrier to re-engineer the immunosuppressive mechanism of a drug (rapamycin) by controlling cellular biodistribution”
Plus I am very comfortable doing TRT via IM. But biology trumped practical issues.
@MAC - All well thought out. I knew you had your reasons and that they were probably backed up by data. Many physicians are starting to use TRT in SQ dosing and getting great responses much of which you have already covered, but trying to avoid the peaks and troughs that may be more valuable in Rapa longevity dosing to avoid immunosuppression. Keep us posted and good luck!
Please define “great responses” re TRT/SQ?
Sure!
Compliance of SQ over IM. Not everyone is up or an IM thigh shot.
Slower and more steady response due to a more even release into the blood stream IM injections tend to get in much faster due to higher vascularity, as you pointed out. Many are dosing twice a week, but some are even dosing daily with small doses.
Less chance of infection causing serious adverse events due to the muscle not being pierced over and over. If an infection occurs sub Q, it will tend to open the skin and not create an issue deep into the muscle.
Overall, most find a very similar response ( some better and some not) with SQ dosing, but with small needles and more likely to self inject vs. have a spouse of other do it for them. Its just alternative option that some people have not been exposed to.
I can see that benefit, especially as I’m currently doing 2 TRT injections + 5 IM rapa injections PER WEEK.
My next iteration is to make an even more super concentrated rapamycin/DSMO liquid, say 60 mg/mL, so I can reduce dose volume/# injections, still deliver mg dose, and thus reduce penetrations.
Mac,
How are you delivering the
intranasal (IN) solution?
A device or?
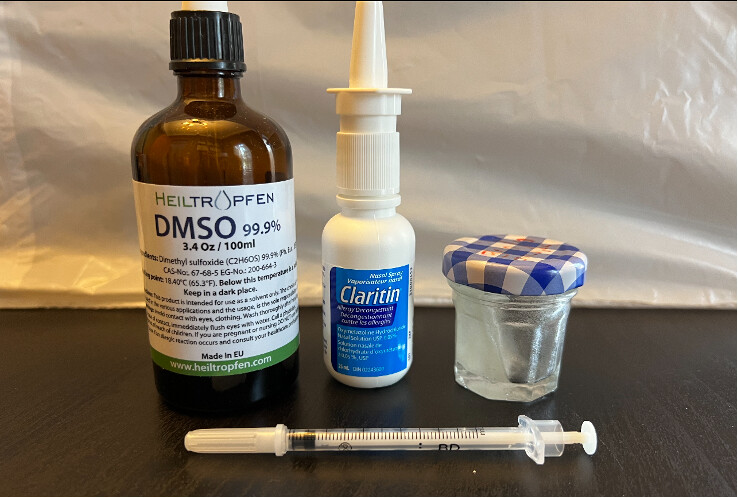
Page 48 of my study. Inside the nasal sprayer is a 30 gm/mL solution of rapamycin in 100% DSMO. You can of course make different concentrations for different volume/dose delivery. You cannot use just “any” nasal spray device…anything that touches DSMO should be INERT to the solvating capability of DSMO. The main storage compartment can be glass. Check for the recycle number under the plastic container and/or ensure the materials used in the mechanical delivery.
Sterilize everything prior to any filling. Keep in freezer. Thaw out prior to use (DSMO solidifies at 19C/65F).
DMSO compatibility with plastics and what kind of jars, sprayers to use
Can DMSO be stored in plastic? Well, yes, but not all plastic types are compatible with DMSO. It is okay to use the below-listed types of plastic.
Dimethyl Sulfoxide is non-reactive to these types of plastic:
These containers are safe to use with dimethyl sulfoxide: