Per my study notes.
Very first full single 0.25mL injection, a large bump developed that was painful (regionally on my injection site leg, and to the touch), which took about a month to dissipate, overlaying ongoing new dosing. In the subsequent weeks, I limited per injection to 0.1mL (total injection volume was split into individual 0.1mL injections spaced apart between both thighs). The 2nd/3rd weeks, the injection sites lingered in terms of residual sting, actually impacted my gait (in combination with the 1st injection large bump which lasted a month); my legs had a stinging feel to them. Per my observations below, it would seem the rapamycin concentration was slowly ramping up as expected without a loading dose (at what we know now is massive dosing) . I was still able to do my daily resistance and aerobic exercise routine, as a reference.
The last few weeks, other than some residual stinging immediately at time of injection, NO lingering pain.
Other than 1st dose bump, NO visible untoward signs of any trauma at the injection site. The bump itself looks totally benign, no discolouration, just a bump in the tissue. Perhaps a small red dot at some sites (blood coming to surface). I did mention in my study notes, blood does aspirate out of some of the injection sites when I withdraw the syringe (not every injection, perhaps 33% of the time). This has NEVER happened with my TRT injections (nor ANY stinging)…so clearly, the DSMO/rapamycin has an entirely different physiological impact on local tissue.
I’ve never done a control DSMO only blank injection to see if the stinging is the DSMO or rapamycin. So I did a 0.1mL DSMO only shot; no stinging, just a tiny rush feeling around the injection site that quickly dissipated.
I took my 5th 15mg/5.8mg IN dose today (feeling fine since last week dose, so onwards). The injections had the characteristic immediate stinging on needle entry…so it’s clearly the rapamycin tissue sensitivity, wow.
But as the weekly doses have progressed, the immediate post injection residual stinging has lessened DRAMATICALLY. Namely, 1st couple of shots, there would be lingering stinging throughout the day/week. As I write this, perhaps 15 minutes have elapsed, I feel next to nothing at injection sites. This was NOT the feeling 1st few doses…they lingered.
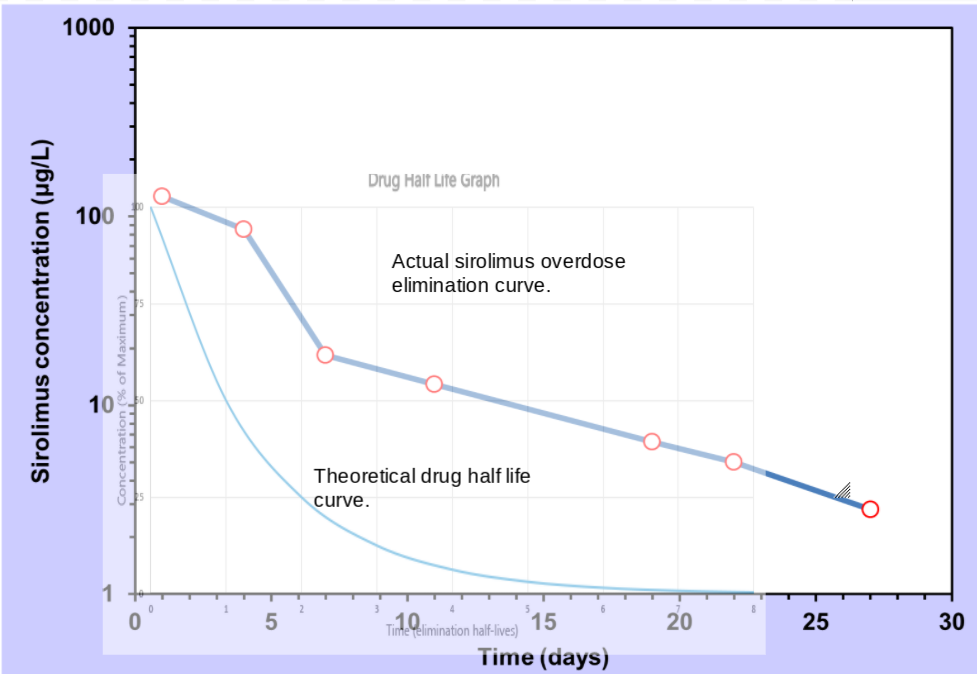
Could this be the significantly elevated residual tissue rapamycin I’ve now built (confirmed by huge trough level) now blunting any NEW rapamycin entry? The tissues are fully sensitized already?
New frontiers…it’s both very exciting but I also wonder if/when the hammer is going to fall. Will a single symptomatic DLT emerge? Will it be the underlying biomarkers going south…deeper into anemia and fatigue, gastro, or infection from WBC depression?
Unlike rodents being injected with rapamycin, at least I can share how I feel with the community…a talking lab rat