I have no idea…I am just starting out in this alternate drug delivery journey. Where I end up, time will tell. I don’t have any expectation that what I do today will be my long term protocol. Hopefully I will be adding some deeper markers with the help of the research community.
Maybe someone will tap me on the shoulder and say they’d like to do mTOR and tissue biopsies, scan my brain and body with radionuclide tracers, etc. I am putting myself out there to learn what is the key that unlocks the escapism.
“The study will be blinded until 3 years after last dog is randomized, at which point we should have definitive answers for primary (lifespan) and secondary (healthspan) endpoints. My current projection is randomization will be completed for all 580 dogs next calendar year. Hopefully closer to June. So definitive answer by mid 2026 hopefully. If effects are big, it’s possible we’ll know something by interim analysis mid-2024, but I think it’s unlikely the effects would be sufficiently positive or negative to unblind at that point.”
MAC:
“You expect primary lifespan endpoint by mid 2026?
I assume each dog has an average intake age and you’d have to run out until a large % of placebo dogs died and significant % of rapamcyin still living re “signal” power? Given the average lifespan of each of these 580 dogs species, how can you have primary by 2026? Perhaps you are screening for this variable?
Sorry, simply assuming most control dogs would live say at least 5 more years before death, how could primary come so early?”
MK:
“Yes, exactly. Dogs have to be at least 7 years old and >20kg at the time of enrollment. In that demographic group, with a cohort size of 580 dogs and three year study period, we should have 90% power to detect a 9% increase in lifespan. That, of course, depends on assumptions from existing mortality data for dogs in that age/weight range, but that’s about the best we have to go on. Among big dogs older than 7 years of age, a significant fraction should reach the end of their natural lives in a three year period.
It’s kind of equivalent to starting with people over the age of 60 and doing a 20 or 25 year study.”
“Studies with higher doses of rapamycin, delivered either orally or intraperitoneally, also had beneficial effects on lifespan extension and on cancer incidence (Bitto et al., 2016).”
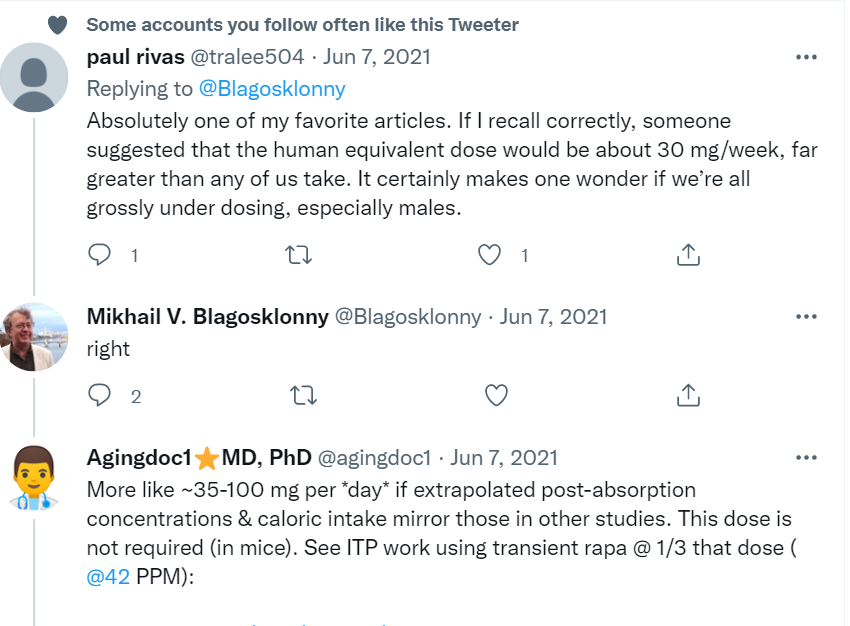
I clearly remember that exchange. At that time I was very swayed by the M Kaeberlein mouse study demonstrating rather extreme life extension using high rapamycin doses, especially in males. I remember emailing Blagosklonny and expressing my concern that we were under dosing the drug in humans. He was in agreement.
But , of course, mice aren’t men and estimates of human translation are from 37-50%. There are multiple reasons for this .
Since then I’ve been wavering in my opinion on dosing based on the low weekly dose of Mannick, and the very low dosing in the prostate prevention trial. In the Mannick study, high doses weren’t superior to low doses.In each case there was evidence of a reversal of immunosenescence, less T cell exhaustion, and improved immunity in actual human trials. Humans trump mice every time and I consider the loss of immune function to be one of the biggest detrimental factors in aging.
So if low dosing is positively impacting one organ system in humans, it’s likely that that’s not an isolated phenomenon, and it’s probably having multiple positive effects. These will most likely lead to a delay in age related diseases and prolong lifespan.
So yeah, I’m changing my mind for the millionth time on dosing and will probably change it again.
I have my hands full managing an entirely new protocol of drug delivery to think about hopping off the train. Besides, for mass uptake and low cost, I’d like to see rapamycin prevail. We are still in the infancy stage of harnessing sirolimus for human lifespan extension.
Took a brief look at Temosirolimus. It’s basically a prodrug of sirolimus…the active metabolite appears to be really sirolimus, but there may be a hybrid mTOR effect at play.
“Our results demonstrate that rapamycin and temsirolimus exert similar in vitro and in vivo anti-proliferative effects against prostate cancer cells. Our results demonstrate that both compounds possess a superimposable pharmacological profile on these prostate cell lines.”
There does not appear to be any “compelling” pharmacological reason to consider it.
It’s FDA approved as an IV delivery (30-60 minutes) version (Torisel, Pfizer) and has some nasty side effects in clinical trials. I don’t read same with sirolimus, so not sure how and why the ADE translation is different between rapalogs.
“An H1 antihistamine should be administered to patients before the start of the intravenous
temsirolimus infusion”
“Pneumocystis jiroveci pneumonia (PJP), including fatalities, has been reported in patients who received temsirolimus. This may be associated with concomitant use of corticosteroids or other immunosuppressive agents. Cases of fatal bowel perforation occurred in patients who received TORISEL. These patients presented with fever, abdominal pain, metabolic acidosis, bloody stools, diarrhea, and/or acute abdomen. Patients should be advised to report promptly any new or worsening abdominal pain or blood in their stools. Cases of rapidly progressive and sometimes fatal acute renal failure not clearly related to disease progression occurred in patients who received TORISEL. Some of these cases were not responsive to dialysis. Patients with central nervous system tumors (primary CNS tumor or metastases) and/or receiving anticoagulation therapy may be at an increased risk of developing intracerebral bleeding including fatal outcomes) while receiving TORISEL.”
A lot of “fatal” outcomes associated with this rapalog and IV delivery. Not sure I want to take this on right now.
So I’ve got massive Sirolimus, my lipids and glucose are CLASSIC mTOR markers, gut microbiome alteration, anemic, but yet I’ve got no MTOR inhibition? I don’t believe it.
“Rapamycin was obtained from LC Laboratories (Woburn, Massachusetts, USA), dissolved in dimethyl sulphoxide (DMSO) at 25 mg/ml and stored at −20°C. For injection, the stock solution was diluted in phosphate buffered saline (PBS). Mice received daily intraperitoneal injections of rapamycin at 1 mg/kg body weight/dose in a total injection volume of 0.3 ml for 10 weeks and control animals received the DMSO vehicle at 0.4% in a total injection volume of 0.3 ml”
Some additional interesting properties of DSMO as my carrier.
And here’s another magical property of DSMO…perhaps of huge benefit getting Rapamycin thoroughly inside body tissue, something far more difficult with plain oral delivery?
“In the body, DMSO can pass through cell membranes as readily as water does without damaging the tissues, and it can replace water molecules within many bodily fluids. And, because DMSO so readily dissolves other molecules, it can also carry them through the cell membranes with it. “DMSO alters cell membrane permeability,” says Jacob. “It moves through membranes and substitutes for water so that it pulls substances through cells that ordinarily would not move through them. This is its basic mechanism of action.”
“Dimethyl Sulfoxide (DMSO) in Trauma and Disease” by Stanley W. Jacob and
Jack C. de la Torre
The book on DMSO
Selected Contents
Chemistry of DMSO. DMSO in Basic Pharmacology. DMSO Clinical Pharmacology.
DMSO in Genetics. DMSO in Basic Microbiology. DMSO in Clinical Microbiology.
DMSO in Malignancy. DMSO in Basic Neuroprotection. DMSO in Clinical
Neuroprotection
You know - I might give Fabio a run for his money on this hair thing. My hair is getting real “purty”, soft and silky. Amazingly rich in color and shine. LOL.
So I had my first post IM+IN rapamycin doc consult yesterday.
On lipids, of course, some concern…but he’s deferring to my upcoming cardiologist consult.
On the anemia, surprisingly sanguine. He figures with my chronic blood donations, my body has adapted to the low iron now (re not being symptomatic or athletic diminution). He use to consternate before I blew by his red line “not < 80 ferritin” a long time ago. TRT also stimulates red blood cell production, so perhaps an underlying resiliency buffer. Could also be partly my iron genes.
On the rapamycin, I had to explain the markers rise was entirely from the recent intervention, including the PSA (he didn’t know what to make of the blip either). Also deferring to my urologist, once I have more duration/transiency data. He knew I started experimenting with rapamycin last year. He knows a little about rapamycin (thank god for Attia…doc says if Attia’s taking it, it must be ok!). His biggest concern is immunosuppression, so he’s adding a deep biomarker panel to capture. As well, more short term markers followup tracking testing (1 month, 3 month) including more sirolimus levels. He didn’t even chastise me for the IM+IN vs oral.