I took my first 3.5mg dose this morning (at least a half hour before any food). Cutting the pill in half is easy, but quartering it is a little more challenging. I felt bloated during the day and did not feel my usual hunger between meals, but saw no other effect. I trust the bloating will decrease over time.
1 Like
I’ve been taking 3 mg for almost a month. I have not experienced any change in weight or hunger
3mg every day, of once a week?
Yeah branded/patented med pricing generally sucks here if one is not “poor” enough for patient assistance programs for medically necessary drugs and doesn’t have excellent insurance (my partner’s Cadillac plan covers an insane amount of stuff including $800/hr cash pay psychiatrist and really expensive branded drugs while corp perks include several free IVFs if needed) - so basically a lot of people in the middle are screwed - but I’ll note on the bright side - generics are actually much cheaper here so a Teva generic of liraglutide will be hella cheap. That being said, it is common for weight regain (most do get some mild longer-term benefit) and in some people, they might even have a huge rebound weight.
I’d be wary of semaglutide from non-legit sources - the TikTok/Instagram crowd is buying them up for non-medical use to the point it is way too profitable to counterfeit/bootleg with questionable quality/safety.
2 Likes
The New York Times: Those Weight Loss Drugs May Do a Number on Your Face.
Ms. Berger was thrilled with her new body. There was, however, a major downside to losing the weight so quickly. Her face suddenly looked gaunt.
“I remember looking in the mirror, and it was almost like I didn’t even recognize myself,” she said. “My body looked great, but my face looked exhausted and old.”
Dr. Oren Tepper, a plastic surgeon in New York, said that it’s common for weight loss to deflate key areas of the face, leading to a more aged appearance. “When it comes to facial aging, fat is typically more friend than foe,” he said. “Weight loss may turn back your biological age, but it tends to turn your facial clock forward.”
2 Likes
Wonderful, so that’s what’s happening.
Ah I have a hunch that extended fasts and/or rapa should be helpful for the “facial aging”
I tend to think you are probably right - I suspect that rapamycin probably prevents many aspects of facial aging because of its maintenance of facial muscle and bone: Three-dimensional Analysis of Modeled Facial Aging
I’ll add there are ways to improve aesthetics and skin health with the following:
Mini-doses of botox when 25-30+ (may reduce somewhat rare antibody formation probability with longer-term use), avoiding sunlight (ROS formation, cytokine signaling, protein oxidation, and mitochondrial damage), the very basic moisturizer/cleanser (reduces transepithelial water loss, & removing air pollution on skin), and using topical tretinoin (increases collagen production, epidermal hyperplasia, decreases keratinocyte/melanocyte atypia) or topical adapalene (as a cheaper alternative with less research but more selectivity for nuclear RAR B-y).
Collagen peptide dietary intake and select cosmeceuticals (some may reduce UV-stimulated MMP activation and improve skin collagen production) are still a maybe in terms of cost-effectiveness.
These are much cheaper than expensive fillers and if we assume skin aesthetics over time lead to slightly higher income (there is a small association) which may be true - these are actually very much cost-effective in that lens.
I do know some people who are interested in testing topical rapamycin for non-photoaging related “skin aging” when an optimized formulation is available with data comparison. It would be nice to know if a specific form of topical rapamycin can actually hit subcutaneous adipose tissue. All we have is topical Retin-A that has limited partial “skin anti-aging” beyond just photoaging.
Especially if it can prove to reduce aging-related frailty of the skin and increase the rate of mesenchymal stem cell differentiation in subcutaneous adipose tissue and improve barrier function over several years of topical application - it might help get rapamycin on the map more so, to be frank.
2 Likes
5 to 7% on a DEXA is bodybuilder-at-competition level. That’s way too low to maintain. Are you sure you don’t mean by calipers (which tend to show about 4-5% lower than DEXA?)
3 Likes
I’m fairly certain Alex means DEXA but note last I checked his publicly posted DEXA - it was T<-2.5. Very low bone density. Also, low lean mass, probably from all that testosterone avoidance.
I’d be very wary of messing with healthspan that much just for a potential theoretical benefit. Too low body fat, worse immune function, more frequent infections, higher risk of fracture, and death are the main concerns.
3 Likes
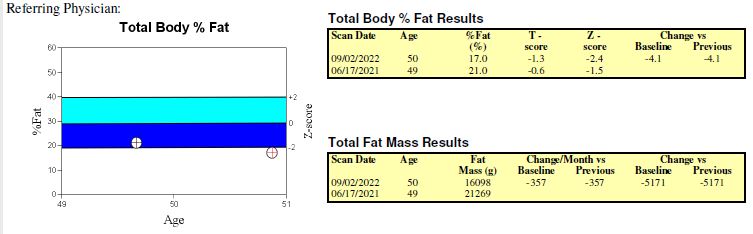
My most recent DEXA Z-score was -2.4, but I’m at 17% bodyfat. That’s Z, not T-score, so it’s based off my age (51), and it’s certainly possible to be in the 5% to 7% range, but that is contest-level lean. Even bodybuilders will go that low only for a day or two.
.
1 Like
I’ll note he is a relatively young age so it’s not that far off.
I’m aware. I went down to 6% once (tested via DEXA) and felt horrible, also had a few bodybuilder buds. Former NASM-certified PT and I’m familiar with exercise physiology. Quite content at 10-12%. 99 percentile bone density age-matched at age 30 with DEXA before starting mild CR and hasn’t dropped so far with mild CR + CR mimetics. And of course, strength training is the big kicker. Having some strength training that spikes T levels is not net harmful.
1 Like
In between those two blood tests, I lost approximately 40lbs.
I’ll have to look back at the inputs and formula on the phenotypic age spreadsheet to see which variables had the biggest effect on my results. I can remember several that would be affected by weight loss as well as the direct effects of GLP-1 drugs, i.e. fasting glucose, CRP (adipose tissue, specifically in the overweight/obese, has been found to throw off all kinds of inflammatory mediators, and GLP-1 drugs have significant anti-inflammatory effects), creatinine (as a surrogate for kidney function, which GLP-1 drugs are known to improve).
1 Like
You were 99 percentile in bone density at 30. Wow! How did you manage that? Do you weight a lot more than average? You must have great genes for bone density.
At my peak, was roughly ~200 lbs and I’m taller than average. I can’t say I have “good genes” on bone density - or at least there isn’t any reason to believe it - in fact, ethnically, associated with higher risk of osteoporosis. My parents don’t have osteoporosis yet but mother has slightly osteopenia
I can’t say for sure exactly what was the cause definitively and it could be related to individual differences too, but here’s what I did that might be related:
Resistance training is probably a large part of it - high-intensity, between the repetitions and %1RM suggestive of strength and hypertrophy, as high volume as possible with adequate rest time spaced out, individualized by muscle group. I used to work out almost every day with 1-2 rest days and ex-NASM CPT. Minimal cardio (45 min 3x week “Zone 2”, no HIIT) at the time due to trouble getting to calorie amounts with too much cardio.
I can go more in-depth on the training regime if you wish, but I’ll just say, in general, there are a huge amount of misconceptions about resistance training in terms of risks, benefits, and implementation if one digs in the literature vs what a good amount of pros are saying, let alone the “bro science” crowd.
Adequate dietary protein (this can get into a complex debate beyond protein synthesis - depends on the intensity and what you’re aiming for - for me personally, I went with slightly under ~1 g/lb bodyweight/day to increase insulin response, theoretical recovery at higher training density, and maintaining a slightly positive nitrogen balance based on my own urine samples with validated biomarkers to avoid error, no need to go excessive on protein - generally right around ~0.8 is cost-effective with high confidence is a good general rule of thumb), calcium (~1000 mg from diet), Vitamin D3 (I took 1,000 IU at the time with minimal sunlight exposure, but now I take 2,000 IU due to slightly lower than what I’d like to hit on an individual level for right around maximal PTH suppression), and no alcohol are the current standards. Potentially, Vitamin K2 - I just ate sufficient amounts of Natto. I ate about 85% “clean” back then but was hard to force the last rough 500 cal or so for ~4,000 cal a day.
I also did CMP, thyroid labs, etc baseline to make sure I wasn’t working against anything metabolic albeit unlikely, and not recommended if one is “healthy” and has no symptoms. Avoiding secondhand smoke and PM2.5 was important too. I also don’t know if this might be related as the evidence is still iffy, but I avoided the use of plastics as much as possible (endocrine disruptors). As for supplements, creatine (Creapure), beta alanine, cycled low dose ephedrine/caffeine for a few years, morning coffee when not on ephedrine, whey protein isolate (with banana post-workout). All NSF certified, so pretty sure no significant contamination or adulteration.
I currently do much less volume for strength training only, but very close to 90%-95%1RM very carefully. I also do HIIT 2x week currently and 1-2x/week Zone 2 when I can fit it in. Mild calorie restriction, low-moderate protein but still significantly above RDA.
I’ll also add since some people tend to be cardio only - but it’s misguided - there are benefits for both and they are independent:
For the older adults here - I did a lot of study on resistance training in older adults, in terms of potential sarcopenia and osteoporosis prevention. Something that might be interesting is ACE inhibitors might enhance a hypertrophic response to strength training (only tested in older adults).
The theory goes it increases skeletal muscle blood flow, higher muscle protein synthesis, increased response in IGF-1 levels, increased muscle mitochondrial density, and decreased inflammatory process overall. See PROGRESS trial. Great if you’re borderline indicated for it. On the other hand, beta blockers might not be a great idea, if there is an equivalent alternative as it blunts the effect. A lot of folks don’t realize how meds blunt exercise in different ways. Finally, if one has menopause or true hypogonadism and any of the commonly prescribed meds that affect BMD then that should also be addressed.
6 Likes
That’s interesting about ACE inhibitors, beta-blockers and muscle hypertrophy. I’m currently transitioning off nebivolol and onto telmisartan (I realize it’s not an ACE but an ARB, hopefully close enough), so I’m eager to see if this has some real-world significance.
I have a bunch of Rybelsus 3 mg samples. I tried taking 1 pill, 2 pills at once and 2 pills an hour apart. No matter what my hunger remains the same with no side effects