Yes it is interesting but I haven’t done it. The juice isn’t worth the squeeze to me as I’m too busy with life but I have to admit I was almost surprised none of you hard corers had picked up that thread.
I can’t link to the whole convo I had with ChatGPT as it’s full of personal data but I am happy to provide more details in screenshots to whomever wants them.
Why is it either or / “vs” - that is interesting, yes - AND having a sense of how much different dosages of rapa impact levels of mTORC1 and mTORC2 would be a gold mine to take out the guessing work that everyone today is doing how high a dose to take while still not being too high?
What are your suggestion for how to currently deal with question like
each individual finding how high he or she can dose rapa / how long washouts need to be / how helpful thing like like acarbose that might help raise mTORC2 are, etc, etc
You could do both if you could measure how much mTORC1 is inhibited. I think it’s more important to validate the therapy rather than measure the dose-response (on mTORC1). There might be some systemic signal since apparently brain mTOR might be inhibited by systemic use, but there’s controversy with this (i.e i’m not sure if TSC tumors which are treated with everolimus are past the BBB, and some study didn’t find any brain mTOR inhibition).
What are your suggestions for how to currently deal with question like
each individual finding how high he or she can dose rapa / how long washouts need to be / how helpful thing like like acarbose that might help raise mTORC2 are, etc, etc
I think you would be putting the cart before the horse. Validating mTORC1 as a biomarker – creating a biomarker – is most important. Then it could be like LDL-C. Or am I wrong here?
If it could be use for retrospective analysis of large datasets on outcomes that would be better but I don’t know if it’s possible as I don’t know anything about it. But yeah if you base on what I know mouse studies and other animals with mTORC1 that’s fine, but if you can measure it in humans, feels like that’s not aiming high enough IMO.
I think maybe you missed the fine print. It was a method for measuring mtorc2 not mtorc1 inhibition that was discussed. Mtorc2 has been very elusive so far to measure and there’s many reasons to steer clear from inhibition.
I don’t think it’s much of a difference either or and the pipeline suggested should be treated as a hypothesis to begin with, i.e not determined to measure something expected in one shot.
Eventually after discussing the matter with ChatGPT it seemed that the easiest proxy to measure would be insulin resistance and glucose spikes — they’re the canary in the mine, followed by an explosion in lipids. So I’m getting me a glucose monitor instead of the fancy mtorc2 lab work.
A few evidence based things that might help while waiting for a targeted solution.
Metformin suppresses TGF-B signaling and reduces NF-kB-driven inflammation, and has direct data showing reduction of pro-fibrotic cytokine expression. It seems to do this at relatively low doses. I take 850 mg, once daily.
Losartan suppresses TGF-β1 signaling; other ARBS do as well but I think Losartan does better and is useful at low doses that do not materially lower BP. Evidence spans cardiac, renal, and hepatic fibrosis. I take telmisartan 80 mg/day.
EPA/DHA reduce TGF-β1 expression, suppress NF-κB, and shift macrophage polarization away from pro-inflammatory phenotypes. I can’t find a marine source that I don’t have some kind of allergic reaction to so I do my best eating fish often.
ROS directly induces IL-11 expression and NAC as a precursor to glutathione is a straightforward intervention. Mouse data (again) show NAC reduces IL-11 in fibrotic lung models. I take 1200-1800 mg/day.
Weaker but decent evidence exists for rapamycin, spermidine, SGLT2i, curcumin, fisetin, and I guess any cocktail known to kill the right senescent cells.
Most of the evidence is intermediated by ROS reduction.
Interesting that you are up for adding another ARB on top of 80mg telmisartan. I too take 80mg/day telmi, but have been researching adding very low dose olmesartan. I’m still pretty deep in the weeds on this, but slowly plugging away.
Re: allergy. Have you tried a very pure EPA only, like “Igennus Pharmepa Restore, Pure EPA”, if you are looking for anti-inflammatory. I take 500mg three times a week. Keep refrigerated (I have a refrigerator solely devoted to medications and supplements).
Have you considered astaxanthin for ROS? In general, there seem to be decent signals with some carotenoids like lutein, zeaxanthin, meso-zeaxanthin and lycopene - macula, brain, CV (atherosclerosis prevention).
I don’t think I will add another ARB to the TM, but maybe keep an eye on it.
I have tried a few purportedly highly refined Omega-3s but have not tried Igennus brand. Thanks for the tip. I’ll try it.
I am taking astaxanthin, lutein, zeaxanthin, and lycopene and guess they go in the mix as well for potentially modulating Il-6 downward. I only mentioned the ones that show up in conjunction with Il-6 studies. I think metformin, ARBs, and maybe NAC are the bigger bets. For years, I had minor lung phlegm production that completely disappeared with NAC. I even have a few reversals to be certain that it is the cause.
I think it’s a judgment call for some of their research. Always follow the motives. Some of the research done on rapamycin is not driven by publication and research grants, but by the desire to cure.
In the longevity space, China is also quite prolific.
Alphabet’s Calico stitches $596M deal for Mabwell’s anti-aging asset
Calico Life Sciences, an Alphabet (Google) longevity biotech, signed an exclusive licensing agreement with Shanghai-based Mabwell Bioscience. The deal, valued up to $596 million, gives Calico global rights (except Greater China) to develop and commercialize Mabwell’s investigational IL-11-targeting monoclonal antibody for age-related diseases. Calico paid a $25 million upfront fee, with potential milestones of $571 million tied to development, regulatory, and commercial outcomes. Mabwell’s drug candidate targets interleukin-11, implicated in aging and fibrotic diseases, and has completed Phase 1 trials in China and Australia.
The official identification for Mabwell’s investigational IL-11-targeting monoclonal antibody is 9MW3811 (also documented as 9MW-3811 ).
Technical Overview
9MW3811 is a high-affinity humanized monoclonal antibody designed to neutralize interleukin-11 (IL-11) by disrupting the formation of the IL-11/IL-11R$\alpha$/gp130 signaling complex. This blockade inhibits the downstream JAK/STAT3 signaling pathway, which is a primary driver of chronic inflammation and fibrotic progression across multiple organ systems.
Application in Age-Related Diseases
While originally investigated for idiopathic pulmonary fibrosis (IPF) and oncology, its application in geroscience was accelerated by research—most notably a 2024 study published in Nature —demonstrating that IL-11 inhibition extends healthspan and lifespan in mammalian models by reducing age-associated fibrosis and metabolic dysfunction.
Key milestones regarding its development for aging include:
Calico Life Sciences Partnership: In June 2025, Mabwell entered into an exclusive licensing agreement with Calico Life Sciences (an Alphabet-backed company specializing in the biology of aging) to develop, manufacture, and commercialize 9MW3811 globally (excluding Greater China) specifically for age-related diseases .
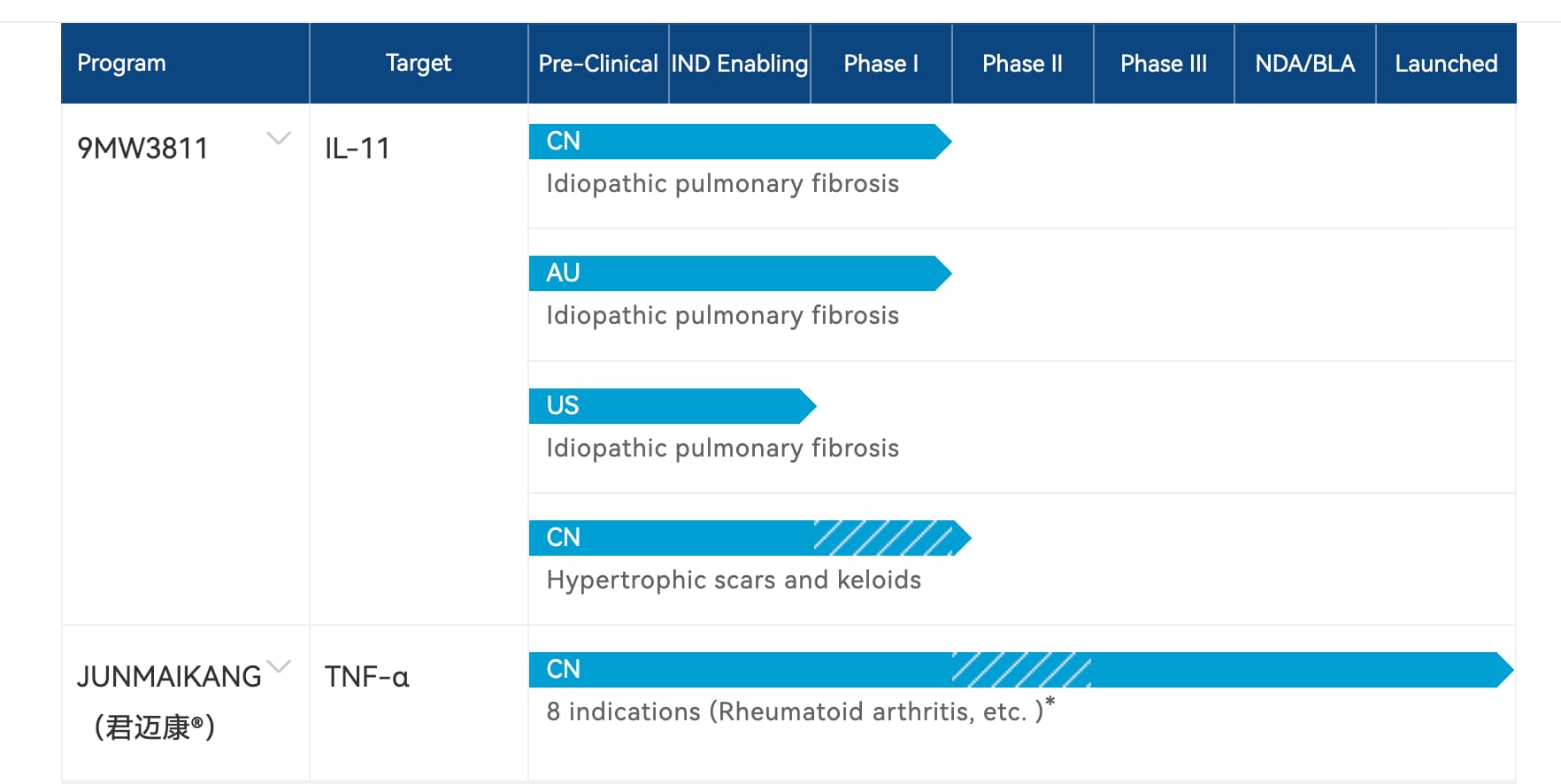
Clinical Status: As of early 2026, 9MW3811 has completed Phase I trials in Australia and China (demonstrating a favorable safety profile and a half-life exceeding one month) and has initiated Phase II clinical trials for indications such as pathological scarring.
Targeted Indications: Beyond general longevity, the compound is being evaluated for its efficacy in multi-organ fibrotic disorders (renal, hepatic, and cardiac), thyroid eye disease, and advanced malignancies.