A lot of longevity treatments reduce inflammation as a side effect so it’s not really the focus.
3 Likes
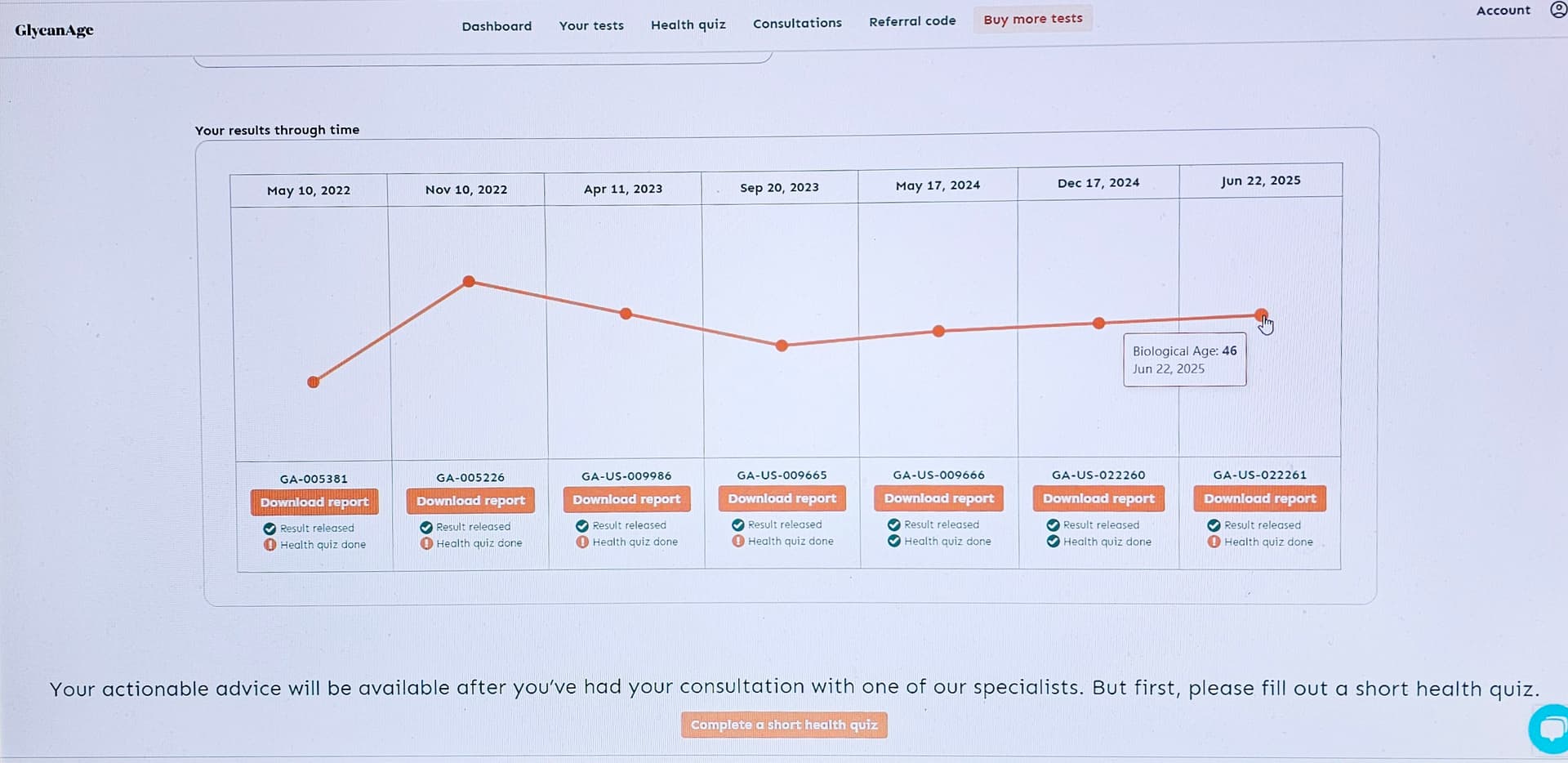
Yes true, rapamycin reduces inflammation and senescence at the cellular level as a target of cell autophagy and repair.
My glycans measurements show that benefit over past 4 years.
4 Likes
So you are saying people are reducing their CRP levels because of their lifestyles and other interventions without directly doing them to lower CRP levels? How many forum members do you think are actually tracking CRP levels as opposed to cholesterol levels, as the CRP is not normally tracked by the basic blood tests that doctors usually prescribe?
Which ones are you referring to? And do you think a large percentage of the forum are doing them?
You need to know your CRP levels to determine if additional interventions are needed reduce CRP levels and what those interventions are.
The problem is there are many things that raise CRP levels, and if you are not measuring CRP levels, you may be at risk without knowing it.
1. Infections
Acute infections are probably the most common cause of a big CRP rise.
- Bacterial infections (pneumonia, cellulitis, urinary tract infections, sepsis, appendicitis, etc.) can push CRP very high (often >50–100 mg/L).
- Viral infections (flu, COVID-19, RSV, etc.) can also raise CRP, but often a bit less than severe bacterial infections on average.
- Chronic infections (like tuberculosis, chronic sinusitis, some dental infections) can keep CRP mildly to moderately elevated for long periods.
2. Chronic inflammatory & autoimmune diseases
These often cause persistent, sometimes fluctuating CRP elevation:
- Rheumatoid arthritis
- Polymyalgia rheumatica
- Systemic lupus erythematosus (SLE) – CRP can be less elevated than you’d expect; ESR is often more sensitive here.
- Inflammatory bowel disease (Crohn’s, ulcerative colitis)
- Vasculitis and other connective tissue diseases
CRP is often used to monitor flare-ups and response to treatment in these conditions.
3. Tissue injury, trauma, and surgery
Anything that causes tissue damage can raise CRP:
- Recent surgery (often peaks around 48 hours afterward)
- Trauma (fractures, major injuries, burns)
- Heart attack (myocardial infarction) – CRP rises as part of the inflammatory response to heart muscle damage.
- Intense muscle injury or rhabdomyolysis
4. Cardiovascular & metabolic risk factors
Even low-grade chronic inflammation shows up as slightly elevated high-sensitivity CRP (hs-CRP):
- Obesity (especially central/visceral fat)
- Metabolic syndrome & insulin resistance
- Poorly controlled type 2 diabetes
- Smoking
- Sedentary lifestyle
- Obstructive sleep apnea
These don’t usually give huge CRP spikes, but hs-CRP in the 2–10 mg/L range can be a marker of increased cardiovascular risk.
5. Cancers
Some cancers, particularly when advanced or causing tissue destruction, can drive up CRP:
- Lymphomas
- Solid tumors (lung, gastrointestinal, etc.)
- Metastatic cancer of many types
Here, CRP is not diagnostic, but can correlate with disease burden or prognosis in some cancers.
6. Chronic organ diseases
Ongoing inflammation or damage in organs can keep CRP elevated:
- Chronic kidney disease
- Chronic liver disease (although severe liver failure may reduce CRP production because the liver makes CRP)
- Chronic lung disease (COPD, bronchiectasis)
- Congestive heart failure, especially when decompensated
7. Lifestyle and other factors
Smaller but real effects:
- Smoking (again—worth mentioning twice)
- Heavy alcohol use
- Periodontal (gum) disease
- Sleep deprivation
- Chronic psychological stress
- Obesity (central role in low-grade inflammation)
These often show up more clearly on hs-CRP than on standard CRP.
8. Medications and medical treatments
Some raise CRP indirectly by causing inflammation:
- Certain drugs that cause hypersensitivity reactions or drug-induced autoimmune syndromes
- Some chemotherapy agents
- Radiation therapy (by causing tissue damage)
Others tend to lower CRP over time:
- Statins
- Some anti-inflammatory biologics (TNF-α inhibitors, IL-6 inhibitors)
- Aspirin and NSAIDs (modestly, in chronic use)
3 Likes
I think this may be somewhat correct, for the simple reason that heart disease / cardiovascular disease is the #1 killer of people in the developed world right now, lipid levels are commonly measured, and we have quite well proven ways to mitigate them.
We don’t have any numbers on how many people die each year from “inflammation”, to the best of my knowledge.
And, while Inflammation is a focus of mine, for example, and I have a HS-CRP measure of about 0.3, which is fine for now, but other measures like IL-6, IL-11, etc are more difficult and more expensive to get, and the precise actions we may want to take to lower age-related inflammation are more complex and unclear. There are no statin-like equivalents (or ezetimibe, PKSQ9 inhibitors, etc.) for inflammation.
So, I would agree, yes, it’s very important, but action plans (beyond staying “healthy” and getting in shape / exercising regularly, eating a “non-inflammatory diet”, etc. - are not so clear cut.
5 Likes
Going forward, I think this is the area we want to focus on, and why I think the Irisin productization will be interesting and important: Long-Acting Irisin With 30-Fold Longer Half-Life has Potent Anti-Inflammatory Effects
So, if we assume most of us here are pursuing the low hanging fruit in the area of inflammation (diet, exercise, etc,) the issue becomes “what’s next?” what are the new things coming down the pipe in the way of therapeutics that may help with inflammation. What will be the PCSK9 inhibitors of the inflammation world?
So I did this prompt:
Identify all the anti-inflammatory biologics (TNF-α inhibitors, IL-6 inhibitors) and also any clinical or scientific research suggesting that if healthy older animals people took these drugs it may improve healthspan and lifespan
Here is what CGPT5.1 came back with:
3. What happens when you give these drugs to aging but otherwise healthy animals?
3.1 TNF-α blockade
Sarcopenia and survival (etanercept, aging mice)
Sciorati et al. (2020, Aging) treated C57BL/6 mice from 16 to 28 months with a TNF-blocking regimen (etanercept). Key results:
- Prevented age-related loss of muscle mass and fiber size.
- Preserved grip strength and performance in hanging-wire tests.
- Reported improved overall survival vs controls (better late-life survival curves, though not a huge lifespan revolution). Aging-US
Paper: “Pharmacological blockade of TNFα prevents sarcopenia…”.
Gut motility / constipation (etanercept, old mice)
- Patel et al. (Sci Rep 2017): old mice show decreased colonic SERT expression, altered mucosal 5-HT, and reduced fecal output. Chronic etanercept in old mice:
- Restored SERT expression and mucosal 5-HT signaling.
- Normalized fecal pellet output and water content. Nature+2Wiley Online Library+2
Cognitive function and cerebrovascular aging (etanercept, aged rats)
- Gocmez et al. (2020, Physiol Behav): 24-month-old rats treated with etanercept:
- Improved performance in memory tasks vs untreated aged rats.
- Reduced peripheral and neuroinflammation, improved endothelial function and hippocampal BDNF levels. PubMed+2avesis.kocaeli.edu.tr+2
Paper: “Etanercept improves aging-induced cognitive deficits…”.
Neurodegeneration models (tauopathy / AD-like)
- In PS19 tauopathy mice, chronic etanercept or a brain-penetrant TNFR fusion reduced microgliosis, phosphorylated tau, and hippocampal neuron loss; behavior improved but this is a disease model, not normal aging. BioMed Central+1
– Ou et al., J Neuroinflammation 2021.
Bottom line for TNF in “healthy” aging animals
In naturally aged rodents, chronic TNF blockade:
- Improves functional aging phenotypes (muscle strength, bowel function, cognition).
- At least one study reports a modest survival benefit when started at mid-life.
- These are small, lab-mouse studies with chronic injections; no multi-species or large-scale replication yet.
5. Direct answer to your question
Are there clinical or scientific data suggesting that TNF- or IL-6-blocking biologics could improve healthspan or lifespan in healthy older animals or people?
Animals
-
TNF blockade (especially etanercept)
- In naturally aged rodents, chronic TNF inhibition can:
- Preserve muscle mass and strength,
- Improve bowel motility,
- Improve cognitive performance,
- And, in at least one study, modestly improve survival when started in mid-life.
- That is legitimate healthspan improvement with suggestive lifespan benefit, but from small, single-lab studies.
- In naturally aged rodents, chronic TNF inhibition can:
-
IL-6 blockade
- No convincing data yet that IL-6 or IL-6R antibodies extend lifespan in otherwise healthy animals. Nearly all work is in disease models.
-
IL-11 blockade (IL-6 family, but not TNF/IL-6 per se)
- Strong mouse data: genetic or pharmacologic IL-11 inhibition from mid-life extends lifespan by ~20–25% and improves multi-organ aging phenotypes.
Humans
- There are no trials giving TNF- or IL-6-blocking biologics to healthy older adults to improve healthspan or lifespan.
- Indirect evidence from RA and other inflammatory diseases suggests:
- TNF inhibitors do not increase overall mortality and may reduce cardiovascular events and Alzheimer’s risk compared with no biologic or csDMARDs, in inflamed patients.
- IL-6 inhibitors effectively suppress inflammation and may increase lean mass in some RA cohorts, but with mixed cardiometabolic signals.
Translating that to primary prevention in healthy aging is speculative and, at present, unjustified given infection and malignancy risks.
Full ChatGPT Response:
4 Likes
At the end of the day, both low CRP and low ApoB should be targeted. It’s not either/or.
Same can be said for blood pressure, Cystatin-C, GGT, A1C, and a few other biomarkers.
We can argue where to rank all of these in the hierarchy of which is most important, but there is really no excuse not to optimize all of these simultaneously. I think everyone would agree on that.
7 Likes
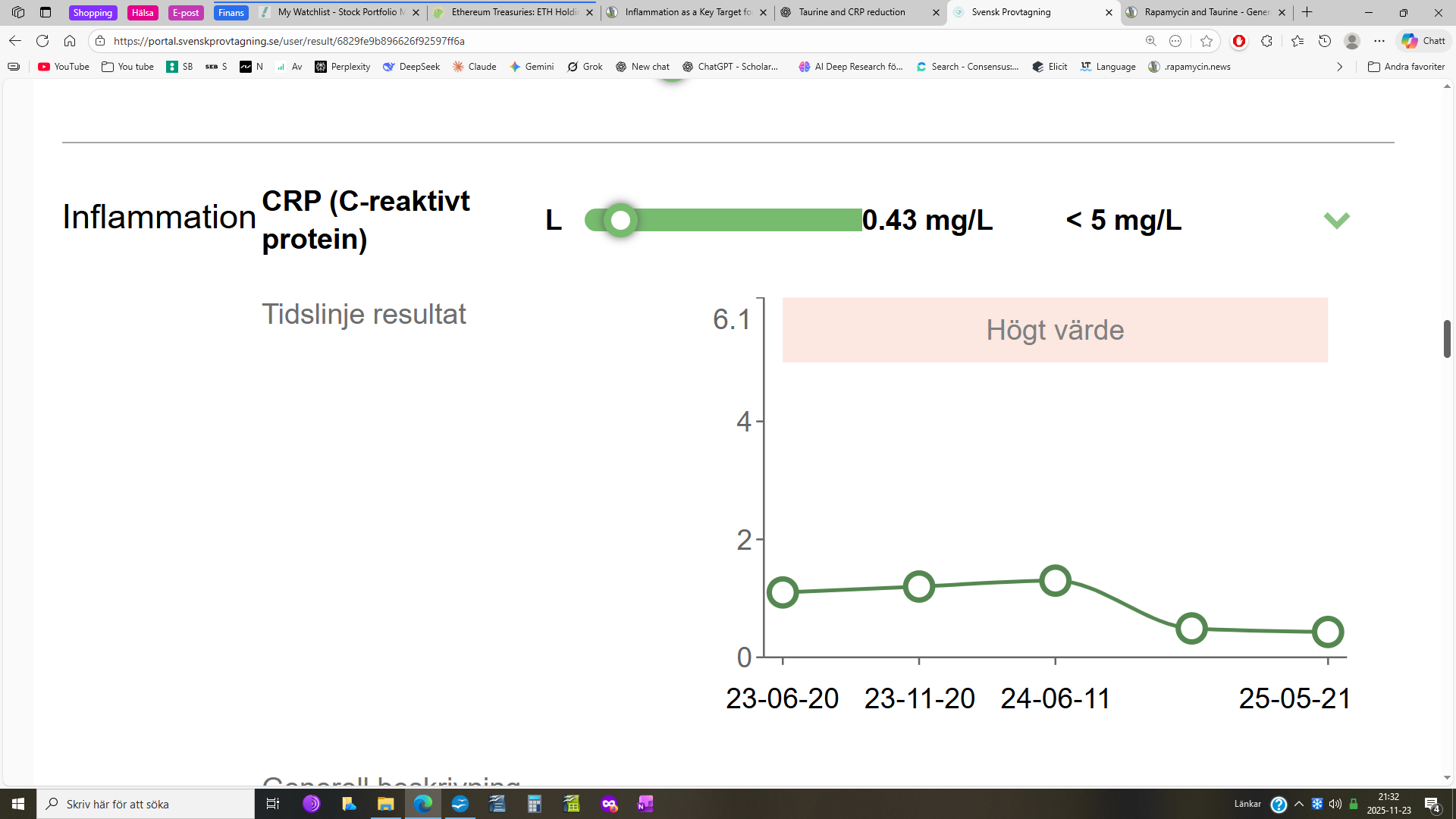
Since I began taking high-dose taurine, my CRP levels have shown a clear downward trend.
- 2023-06-20: 1.1 mg/L
- 2023-11-20: 1.2 mg/L
- 2024-06-20: 1.3 mg/L
I started high-dose taurine in May 2024, taking 10 grams per day, all at once in the morning.
After about seven months on this regimen:
- 2024-12-09: CRP dropped to 0.49 mg/L
- 2025-05-21: CRP was 0.43 mg/L
Since then, I’ve taken a break from rapamycin and recently restarted at 6 mg/week (Rapamune). I’ve also reduced taurine to 5–6 grams per day. I plan to recheck CRP in the coming weeks.
So what caused the drop? Taurine is my prime suspect — it was the only major change I made before my CRP levels fell sharply — but it’s still unclear whether it’s taurine alone or a combination of factors.
5 Likes
It’s clear that inflammation is a significant factor in aging and lifespan, not to mention quality of life, for which maintaining good vision is priceless
Reducing inflammation may protect against early age-related macular degeneration-like vision loss
This is not really new information: The following reference is from 2005.
Progression of Age-Related Macular Degeneration: Prospective Assessment of C-Reactive Protein, Interleukin 6, and Other Cardiovascular Biomarkers | Cardiology | JAMA Ophthalmology | JAMA Network
wherein it is suggested that a CRP level greater than 0.5 is associated with at least a 3x greater rate of progession of ARMD
As is supported by:
Increased systemic CRP associated with choroidal thinning in intermediate ARMD
chen-rachel-increased-systemic-c-reactive.pdf
Additionally; regarding heart disease
Inflammation now predicts heart disease better than cholesterol | Empirical Health
Which is recognized by the American College of Cardiology
Inflammation and Cardiovascular Disease: 2025 ACC Scientific Statement: A Report of the American College of Cardiology - PubMed
3 Likes
If low-dose colchicine is good, febuxostat is better. Uric acid is itself inflammatory, and it spreads inflammation throughout the body. Allopurinol didn’t work for me, but febuxostat probably saved me from needing surgery.
1 Like
I’m seriously considering the COR One device from Cor Health.
The COR One™ device by COR Health is an at-home, FDA-registered medical device designed to track and measure chronic, acute, and low-grade inflammation using just a single drop of blood. Here are the key details:
- What it measures: The device analyzes your Erythrocyte Sedimentation Rate (ESR), a sensitive inflammation biomarker often used to track “silent” or chronic inflammation. ESR has greater sensitivity at low ranges compared to traditional hs-CRP tests, making it suitable for monitoring ongoing inflammatory states, lifestyle effects, or therapy/supplement changes.
- How it works: You use a tiny blood sample (via a painless prick). Results are typically available in 30 minutes and can be viewed in a companion app or dashboard, allowing you to spot trends and understand how diet, activity, or supplements impact your inflammation.
- Intended benefits: Provides personalized insights, allows for frequent monitoring without lab visits, and can help optimize your health plan (nutrition, workouts) based on inflammation data. Featured user stories mention optimization of diets and workouts as well as tracking the effect
4 Likes
I really think there is a progressive inflammatory process that is the debilitating factor in ageing. Multiple processes and pathways no doubt and difficult to identify all. The device isn’t expensive so, a useful tool with no downside. I’ve taken many supposed anti-inflammation supplements over the years but never really felt any different and no tool available to evaluate response. Let us know what you think if you get it, Steve.
3 Likes
I think that would be great.
Amazon has cholesterol test meter kits. I don’t know how good they are, as they get mixed reviews.
“5 Cholesterol results (Total, Triglyceride, HDL, LDL and TC/HDL). High quality test results”
So now we can do CGT, sleep quality (Oura Ring), COR One inflammation testing, glucose, LDL, testing, etc., at home.
Maybe in the near future someone will produce an all-in-one home blood testing device.
I don’t think that is overkill. It would be nice to track what some of our diets, supplements, and meds are doing on a more frequent basis than annual or semi-annual lab blood testing.
1 Like
This Cdn company is working on a home blood testing device
Meet Vi
Experience fast, convenient home health monitoring with the Vi device from Verv. Designed to test and track key biomarkers right from your home, Vi eliminates the need for lab appointments and provides essential health data with ease. Obtain accurate biomarker readouts without ever stepping into a lab. Our mission is to simplify advanced sample-to-result home health monitoring, making it accessible and convenient. Discover deeper insights* into your health with Vi.
3 Likes
Have read that inflammation rises with aging. Are there goals or targets, by age and by gender?
I am 76. My most recent HSCRP is 1.8 and I am thinking it should be considerably lower. Am already focusing on it through exercise, diet, hot whirlpool/cold swimming pool, and not sure what else to do, short of meds like colchicine.
What is an “acceptably good” level for a female my age? My APOB is 49 (I’m on Repatha and Exetimibe) and Chol/HDL ratio is 1.5 as trigs are low (66) and HDL about 117.
Would appreciate pointers to research that suggests targets.
2 Likes
Good question. Here is what I found.
Short answer: there is no formally agreed “optimal by age” panel for inflammation and longevity. What we do have are:
- (a) markers with strong prospective data linking them to CVD, disability, and mortality
- (b) cut-points where risk curves clearly worsen
- (c) age-related drifts that are probably not benign (“inflammaging”).
Summary table (all values approximate)
| Marker (units) | Longevity-oriented target (20–40y) | 40–60y | 60–80y | Rationale (evidence + extrapolation) |
|---|---|---|---|---|
| hs-CRP (mg/L) | 0.2–0.7, consistently <1 | <1, ideally 0.3–0.9 | <1.5, ideally <1 | CDC/AHA define <1 as low CVD risk; 1–3 intermediate; >3 high, with many cohorts showing monotonic risk above ~1 mg/L. Successful-aging cohorts have CRP toward the low end of population distributions. |
| IL-6 (pg/mL) | ≤1.5(ideally ≲1.0) | ≤2.0 | ≤2.5–3.0 | Meta-analysis of “healthy” adults shows mean ≈5.2 pg/mL but with clear age-related drift and wide skew. In older cohorts, IL-6 ≥~3.2–3.5 pg/mL (top quartile) ≈ 2× mortality and sharply lower odds of “successful aging.” Lab reference upper limits (~5–7 pg/mL) appear too permissive for longevity. |
| GlycA (µmol/L) | ≈300–350 | ≈325–375 | ≈350–400 | Reference interval in healthy adults ~273–487 µmol/L; mean in middle-aged cohorts ≈370–380. Labcorp uses <400 as “low risk.” Higher GlycA predicts CVD, diabetes, and all-cause mortality; risk appears graded above ~400. |
| NLR (ratio) | 1.0–1.8 | 1.0–2.0 | 1.0–2.2 | General and disease-specific cohorts show non-linear mortality risk rising from ~2.0 upward; NLR >2.05 or >3.0 is repeatedly associated with worse survival and higher CVD risk. Aiming for ~1–2 seems reasonable when not acutely ill. |
| Total WBC (×10⁹/L) | 4.0–6.0 | 4.0–6.5 | 4.0–7.0 | Higher WBC within the 4–10 “normal range” predicts CHD and all-cause mortality; those at 6–10k have ≈30–40% higher mortality vs ~3.5–6.25k. Values <3.5 can signal marrow or immune problems, so “low-normal” rather than suppressed is the target. |
| Fibrinogen (mg/dL) | 200–300 | 200–325 | 225–350 | Standard reference 200–400 mg/dL; CVD risk roughly doubles per 100 mg/dL increment across large meta-analysis. Thus aiming for the lower half of the normal range, while avoiding hypofibrinogenemia, is sensible. |
| Albumin (g/dL) | ≥4.5 (up to ~5.0) | ≥4.3–4.5 | ≥4.2–4.3 if feasible | Multiple cohorts show monotonic risk: lower albumin predicts higher all-cause and CVD mortality, even within “normal” ranges, with steep risk below ~3.5–3.8 g/dL and incremental benefit up to at least mid-4s. Age-related declines are common but appear maladaptive rather than benign. |
Again: age columns for IL-6, GlycA, NLR, fibrinogen, and albumin are informed extrapolations, not validated targets.
3. How to interpret this in practice
3.1. “Green zone” vs “watch zone” (simplified)
For a generally healthy adult (no acute infection):
-
Clearly favorable / “green” (all ages)
- hs-CRP: <0.7 mg/L
- IL-6: ≤1.5–2 pg/mL
- GlycA: <350–375 µmol/L
- NLR: ≈1–2
- WBC: ≈4–6.5 ×10⁹/L
- Fibrinogen: ≈200–300 mg/dL
- Albumin: ≥4.3–4.5 g/dL
-
“Watch / investigate” (outside acute illness)
- hs-CRP ≥2 mg/L, especially if persistent on repeat testing.
- IL-6 ≥3 pg/mL on multiple occasions.
- GlycA ≥400 µmol/L .
- NLR >2.0 chronically, especially >3.0 without clear acute stressor.
- WBC at the high-normal end (>8–9 ×10⁹/L) chronically.
- Fibrinogen >350–400 mg/dL persistently.
- Albumin <4.0 g/dL, unless clear reversible cause (e.g., acute illness, nephrotic loss, malnutrition).
The pattern across markers matters more than any single value.
4. Age effects and “realistic” vs “ideal”
Empirical reality: IL-6, CRP, NLR, and fibrinogen do rise with age on average; albumin tends to fall. That is the biochemical signature of inflammaging.
But: Cohorts of “successful agers” (preserved function, low burden of disease) typically sit closer to “younger-adult” values of IL-6 and CRP than to their age-matched peers.
So there are two ways to use age in targeting:
- Strict approach (longevity-maximalist)
- Try to keep markers in the young-adult green zone for as long as possible (e.g., IL-6 ~1–2, hs-CRP ~0.3–0.7, NLR ~1–2), assuming no immunodeficiency or frailty.
- Realistic approach (frailty-aware)
- In advanced age or multi-morbidity, accept slightly higher “acceptable” ceilings (e.g., IL-6 up to ~3 pg/mL, hs-CRP up to ~1.5), focusing more on preventing further upward drift and supporting function rather than forcing numbers “back to 25-year-old levels.”
There is no evidence that pushing these markers below the low-normal range (e.g., hs-CRP ~0, IL-6 almost undetectable) further improves longevity, and it could plausibly impair host defense.
Full CGPT Response
2 Likes
And some ideas for how we can get, or keep, our measures into the optimal range:
Below is a concise, mechanistically grounded, high-impact set of interventions—prioritized by effect size and evidence quality—for each inflammation marker you listed. Embedded links point to primary literature or high-quality reviews.
1. hs-CRP (chronic, non-infectious)
Target: <0.5 mg/L for longevity; <1.0 mg/L acceptable.
Highest-impact levers
Lifestyle / behavior
-
Adiposity reduction (esp. visceral fat) — the single most powerful non-pharmacologic CRP reduction. CRP declines ~0.5–2.5 mg/L with weight loss depending on baseline obesity.
• Review: https://www.nature.com/articles/ijo2017131 -
Aerobic exercise — regular moderate/higher-intensity reduces CRP ~20–40%.
• Meta-analysis: https://bjsm.bmj.com/content/45/6/468 -
Sleep optimization — sleep restriction elevates CRP; 8 h/night normalized it.
• NEJM-related review: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5449130/
Dietary levers
-
Mediterranean-pattern diet — consistent CRP lowering independent of weight loss.
• PREDIMED: https://www.nejm.org/doi/full/10.1056/NEJMoa1800389 -
High-polyphenol EVOO (oleocanthal-rich) — acute NSAID-like COX inhibition + chronic CRP reduction.
• Clinical: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4682605/
Supplements
-
Omega-3 EPA/DHA (2–4 g/day) — reduces CRP ~20–30%; dose-responsive.
• Meta-analysis: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6358920/ -
Berberine (500–1500 mg/day) — CRP reduction independent of glucose effects.
• Meta-analysis: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8061759/ -
Curcumin (≥1 g/day, high-bioavailability forms) — ~0.5–1 mg/L CRP drop.
• Meta-analysis: https://pubmed.ncbi.nlm.nih.gov/29713141/
Drugs
-
Statins (rosuvastatin strongest) — CRP reduction independent of LDL lowering; ~30–50%.
• JUPITER: https://www.nejm.org/doi/full/10.1056/NEJMoa0807646 -
SGLT2 inhibitors — consistent CRP and IL-6 reductions and NLR improvement in diabetics and non-diabetics.
• Review: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8653745/ -
Low-dose colchicine (0.5 mg/day) — potent CRP and IL-6 suppression; major CV-risk reduction.
• COLCOT: https://www.nejm.org/doi/full/10.1056/NEJMoa1912388
see the full response for how to optimize all the different inflammation markers:
Also, I recently stumbled upon this:
Anti-inflammatory eating plans like the Mediterranean or DASH diet can fight inflammation in the body, lowering the chance of it contributing to a host of chronic illnesses.
Related:
2 Likes
This seems to be supported by the research:
Yes. There is human evidence that taurine can reduce CRP/hs-CRP, but the data are limited, short-term, and mostly in metabolically unhealthy populations rather than healthy adults.
1. Key human data on taurine and CRP
Randomized clinical trial in type 2 diabetes (T2DM)
- Design: 120 adults with T2DM, randomized to taurine 1.5 g twice daily (3 g/day) + low-calorie diet vs placebo + low-calorie diet for 8 weeks.
- Findings: Compared with placebo, the taurine group had a significant reduction in hs-CRP and other inflammatory/oxidative markers (e.g., MDA), alongside improvements in endothelial markers and insulin resistance. ([BioMed Central][1])
- Paper: “Protective and therapeutic effectiveness of taurine supplementation plus low calorie diet on metabolic parameters and endothelial markers in patients with diabetes mellitus: a randomized clinical trial” – free full text via Nutrition & Metabolism: article.
Systematic review and dose–response meta-analysis
- Study: Faghfouri et al., 2021/2022 systematic review + dose-response meta-analysis of controlled trials of taurine on inflammatory and oxidative stress biomarkers. ([PubMed][2])
- Conclusion: Taurine supplementation significantly decreased CRP and malondialdehyde (MDA), with stronger effects at ~8 weeks of supplementation.
- Access: European Journal of Clinical Nutrition meta-analysis: journal page and an accessible version via ResearchGate: full text link.
Full CGPT response:
2 Likes
Cooling vests do more than cold plunging or cold swimming.
A better, modern clock, Linage2 (LinAge2: providing actionable insights and benchmarking with epigenetic clocks | npj Aging) includes cholesterol, CRP, and several other inflammation indicators.
You are correct though that inflammation is a big player in CVD, and brand new guidelines agree with you. They now say that CRP and other markers should be taken into consideration and targeted for treatment in the same manner as cholesterol: https://www.jacc.org/doi/epdf/10.1016/j.jacc.2025.08.047
The problem is, lowering inflammation is very tricky because it’s so hard to define. CRP, ESR, various cytokines etc are only indicative, and all of them are non-specific. You can also be terribly unhealthy and those markers are totally normal.
I think D-Dimer is another under-rated inflammation marker, as is ferritin. Worth looking at those too IMO.
1 Like