Is there a trusted pharmacy that is typically used?
1 Like
See here:
- Buy Rapamycin Online - List of Reliable Pharmacies
- What Brands of Medications to buy: Generally Good Indian Pharma Companies
2 Likes
Doing further research, I am wondering about drug interactions. For example, what if your version of poor glucose control does not result from any defect in beta cells GSIS, and since one way in which imeglimin works is that it “fixes” GSIS, you may surmise that imeglimin might not be for you. But what if you are also taking another drug, say, sirolimus, which longer term or with some protocols (daily dosing?) actually damages beta-cells GSIS? Now you might be adding this defect to your glucose control issues, and what if under those circumstances (i.e. you taking sirolimus) taking imeglimin might make sense, whereas without sirolimus it does not.
Evidence for Rapamycin Toxicity in Pancreatic β-Cells and a Review of the Underlying Molecular Mechanisms
Quote:
“Overall, the majority of these studies demonstrate significant effects of rapamycin on glucose homeostasis, and the combined evidence strongly suggests that rapamycin adversely affects GSIS from β-cells.”
Of course, GSIS from beta-cells can be impacted through various mechanisms, so it remains to be shown whether imeglimin can “fix” the damage sirolimus does to beta-cells. Again we need to take a closer look at the MOA of both drugs to guess at any possible interaction, and then test it. The research continues.
3 Likes
“suppresses hepatic neoglucogenesis” “fixes GSIS”
Aren’t these good things? GSIS declines with age.
(Gemini)
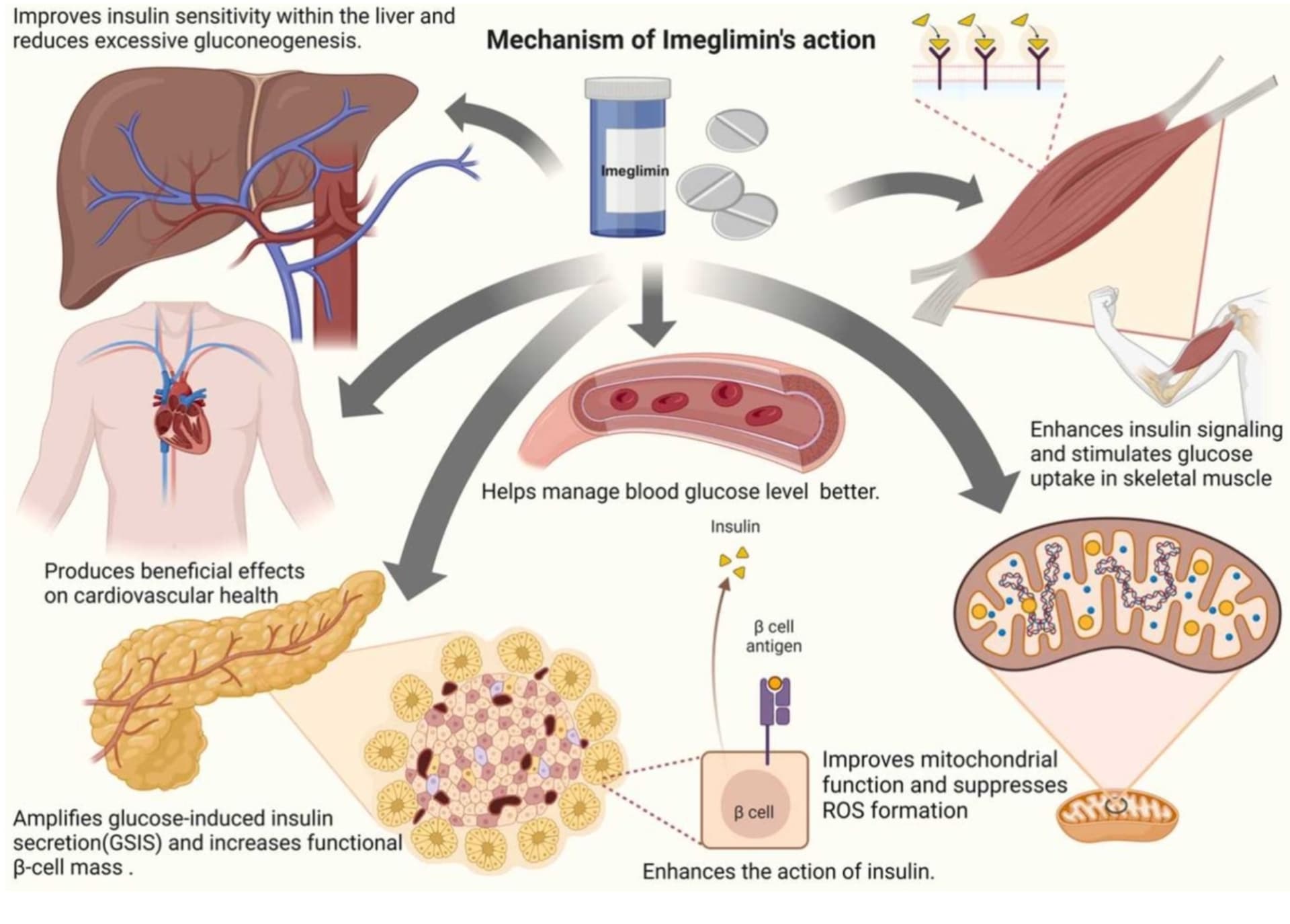
"Yes, Imeglimin suppresses hepatic gluconeogenesis (the production of new glucose by the liver). It is a core part of its “dual-benefit” mechanism of action, which targets the liver, skeletal muscle, and pancreatic beta cells.
Mechanism in the Liver
Imeglimin reduces excessive glucose production through several mitochondrial-dependent pathways:
Mitochondrial Rebalancing: It acts on the mitochondrial respiratory chain by partially and competitively inhibiting Complex I and restoring the activity of Complex III.
Energy Regulation: This rebalancing lowers the ATP/ADP ratio and increases mitochondrial redox potential in hepatocytes, which reduces the driving force for gluconeogenesis."
"Age-Related Decline in GSIS
In humans, beta cell function generally declines with age, estimated at a rate of approximately 1% per year. This decline is often independent of peripheral insulin resistance or body mass index.
Reduced Stimulated Secretion: Islets from younger donors (<40 years) typically exhibit significantly higher GSIS than those from older donors.
Elevated Basal Secretion: Aging is often associated with an increase in basal (fasting) insulin secretion, which may represent a compensatory state but also reduces the cell’s “dynamic range” when stimulated by high glucose.
Mechanisms of Dysfunction."
4 Likes
Apparently in a percentage of users SGLT2i can increase the risk of erythrocytosis (see paper below). If imeglimin prolongs how long erythrocytes persist in the serum, then wouldn’t the concurrent use of both drugs further elevate the risk of erythrocytosis?
From the canagliflozin thread, a paper posted by @Davin8r:
Erythrocytosis and thromboembolic risks associated with SGLT2 inhibitors in type 2 diabetes
1 Like
It certainly could, and would be potentially even worse with testosterone + SGLT2i + imeglemin. T and SGLT2i mainly work by stimulating production of RBC, so if then you add in a drug that reduces RBC senescence/removal then I’d expect to see even more of an increase in hemoglobin/hematocrit.
3 Likes
Then slow titration should be used, with frequent blood draws. And looking for hemo increasing.
1 Like
5 Likes
Have you made any tests? Glucose maybe?
1 Like
I’m starting today. I use a CGM and I take fingerpick glucose every morning.
4 Likes
Fantastic. Super interested in this. Please keep us posted. Also very interested in BG now that you’ve stopped pio, but before you start up on ime otherwise it’ll be hard to disentangle the effects of one vs the other. I think ime is less potent in glucose lowering than metformin, and since met did nothing much for you (did zilch for me), I think if there’s an effect, it’ll really be down to the different MOA.
4 Likes
Well, your reports with numbers will be much appreciated.
Same for me. metformin did not change anything. That said imeglimin has more MOAs than metformin:
(Gemini 3 pro)
Imeglimin does everything Metformin does (sensitizes the body to insulin), but it also stimulates the pancreas to release insulin in response to glucose (Glucose-Stimulated Insulin Secretion, or GSIS).
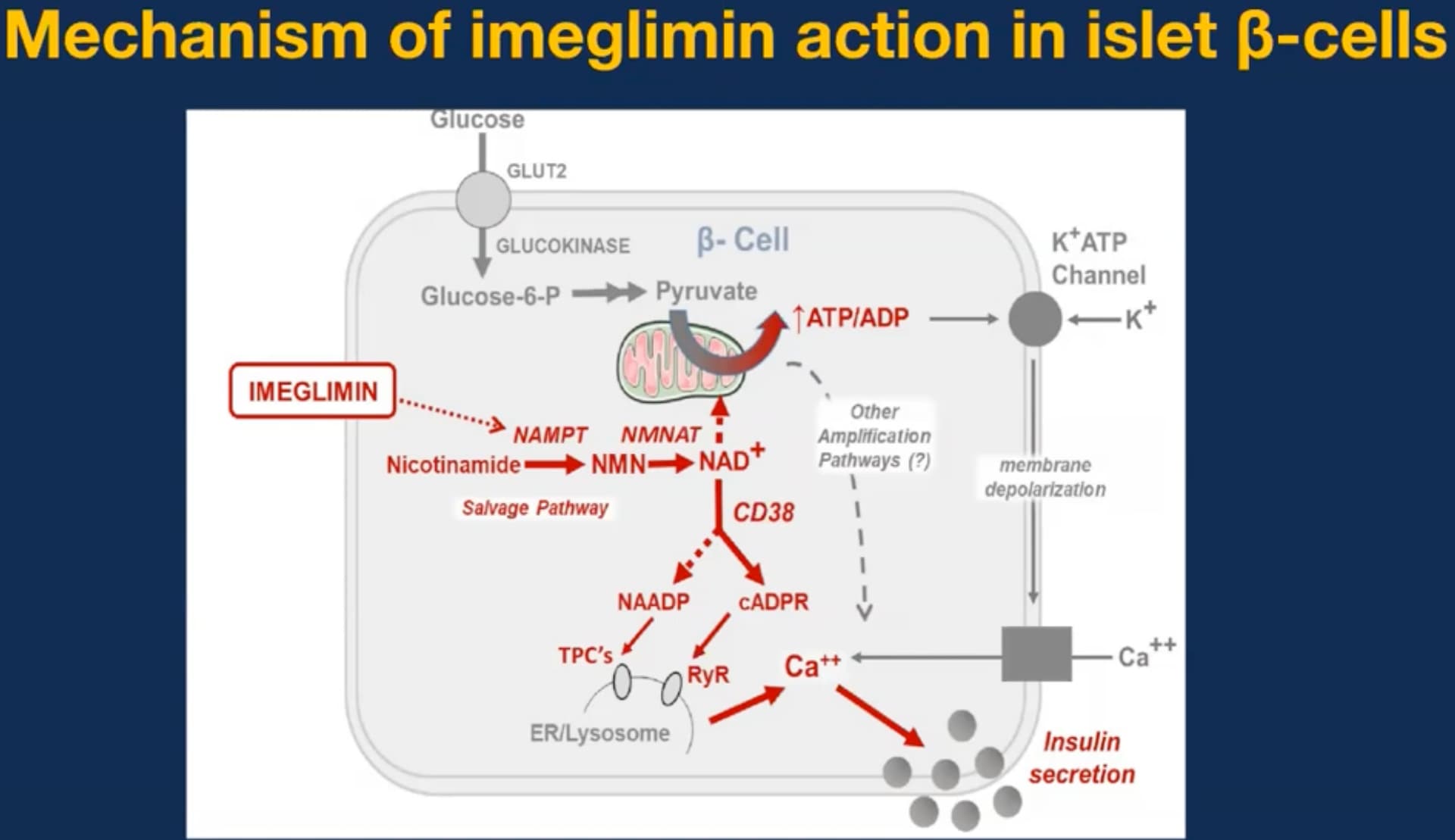
Imeglimin promotes the synthesis of NAD+ (via the salvage pathway). Increased NAD+ leads to higher intracellular calcium levels in pancreatic beta-cells, which is the direct trigger for insulin release.
Imeglimin has been shown to prevent the opening of the Mitochondrial Permeability Transition Pore (mPTP) . When this pore opens, cells die (apoptosis). By keeping it closed, Imeglimin helps preserve pancreatic beta-cell mass, potentially slowing the progression of diabetes.
5 Likes
I ordered the same brand, and it’s on its way. I am hoping it will lower my fasting glucose levels.
Metformin worked fine for me until I developed an intolerance for it.
Glynase and empagliflozin do nothing for me, at least compared to metformin.
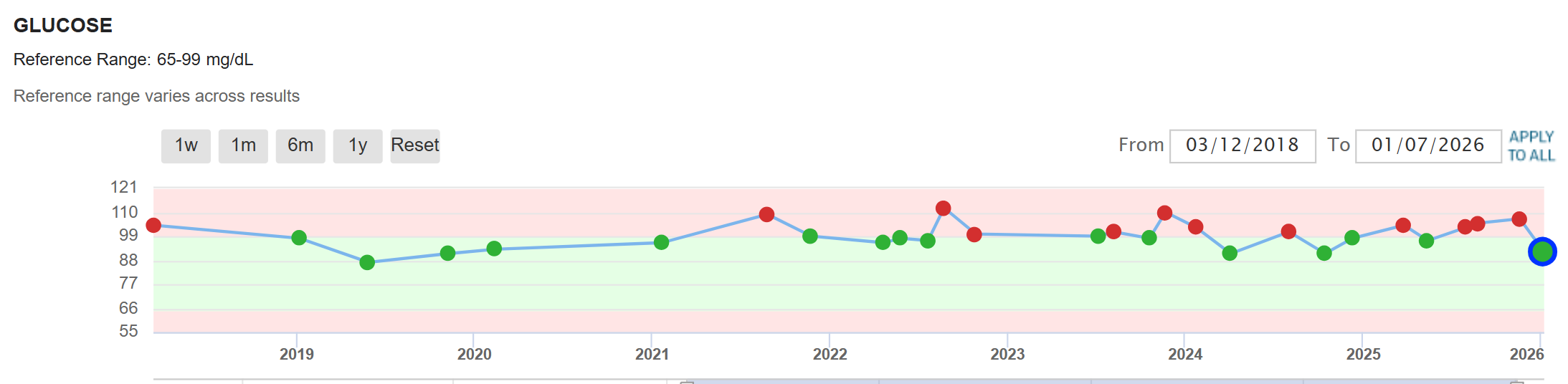
My fasting glucose is suboptimal, which is contrary to the rationale that we want all of our bloodwork to be optimal for longevity. I can lower my fasting glucose by fasting longer than usual and drinking lots of water before my blood test. My own in-home test tells a different story. My morning glucose reading after being up for two hours and fasting for 14 hours is always between 101 and 110. I would like it to be between 90 and 100.
Of course, my doctor is not concerned and will not prescribe further medications until my fasting glucose and A1C become significantly worse. Two doctors have told me that at my age, everything is okay. They are not longevity doctors.
4 Likes
Tracking fasting insulin, and A1c will also be very useful.
3 Likes
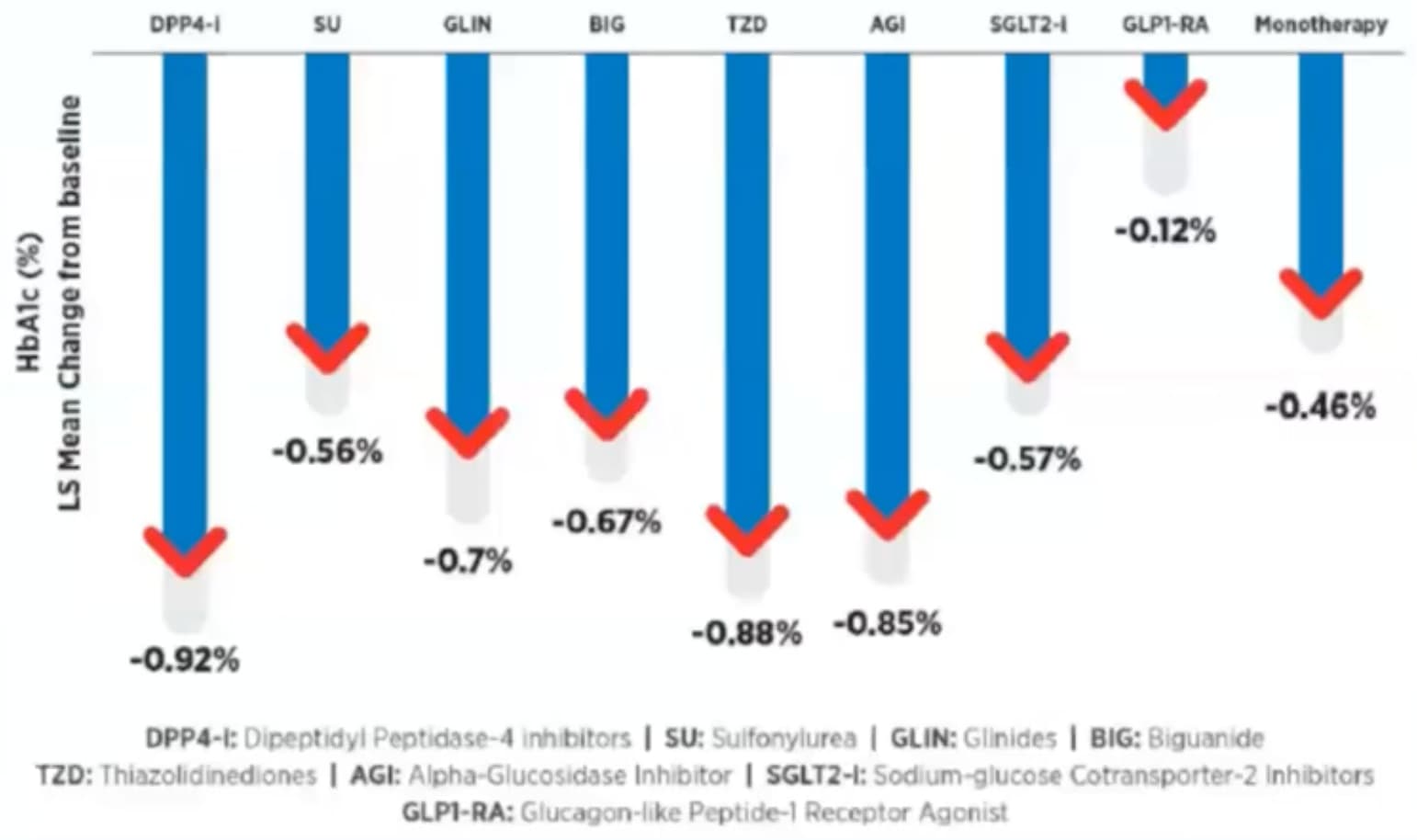
I just watched a video of an Indian talk about Imeglimin with lots of interesting slides such as that one:
(Note all the cool stuff about NAD+, CD38, etc.)
Slightly less cool is that adding it to GLP1-RA does not reduce HbA1C by much.
That said they have theories about why and on the other hand the combination with a SGLT2i is OK.
As usual the effect size is highly dependent on individual variability so I’m hopeful.
The full video is here:
Imeglimin Novel agent in T2D Armamentarium with Dual Benefits
3 Likes
Very cool, tangentially, a new study found that the addition of a GLP1 to metformin was the best, compared to sulfonylureas, SGLT-2is, and DPP-4is for A1c control .

Conclusions: In this target trial emulation, GLP-1RAs were most effective for glycemic control, aligning with GRADE, and superior to SGLT-2is in combination with metformin for T2DM in patients with low-to-moderate cardiovascular risk.
3 Likes
This is not the right thread, but I suspect that people who are classified as prediabetic based on the common criteria of FBG and A1c, are not a uniform group. I suspect, that within that group there is a cohort who are for lack of a better term “pseudo-prediabetic”, meaning that while they meet the biomarker definition, their presentation is different, and in fact is not a diabetic continuum. Those people can have prediabetic levels of FBG and A1c for years if not decades and never transition into diabetes as “true” prediabetics usually do. They don’t spike their BG above 140mg/dL after a meal, but often go much above 100 as a result of exercise. Their dawn effect is high 100-115, but not necessarily during the rest of the day. Their insulin sensitivity is fine, but their liver just keeps pumping out glucose through neoglucogenesis. It is not clear to me if it’s a morbid condition that needs treating like true prediabetes–>diabetes. It’s like with high LDL - it’s bad for most, but there are those who seem protected in some way, despite lifelong high LDL have zero atherosclerosis.
If - and that’s a big if - that is a correct hypothesis, then the question becomes: should those people still try to lower their FSB and A1c, and if so, should they use drugs that were designed for diabetes, even if they don’t necessarily have the same MOA operating for them (this is where imeglimin comes in). Or maybe this is all pointless speculation.
3 Likes
As I’m in the same camp I looked at that in the past and the conclusion was that it’s pretty bad anyway. That’s why I’m still trying to reduce my glucose to normal levels.
Out of convenience here is Gemini 3 pro’s take on that:
5 Likes
Yeah, ultimately I also decided that it’s likely better to normalize glucose handling into a more optimal range. Now it’s a matter of finding the right drug regimen. I’m looking forward to your ime reports.
3 Likes