Certainly a valid concern. However, it is super important to try to understand the MOA (mechanism of action) of any drug before making a decision about taking it. There are drugs that increase insulin output, such as sulfonylureas, meglitinides, glp-1ra etc. However, you have to ask about the MOA of any particular class of drugs. If the drugs force greater insulin output from beta cells leading to beta cell exhaution, that can be a long term negative. But what if your pancreas would release a “normal” amount of insulin in response to glucose levels, but it’s prevented by some kind of defect in some beta cell pathway, either production or release or whatever. Then, removing that defect simply restores insulin levels to “normal” - in that scenario increased insulin levels are not a negative.
That’s why it is so crucial to try to establish the MOA. But let us assume that imeglimin increases insulin production through repairing a defect along the beta cell pathway.
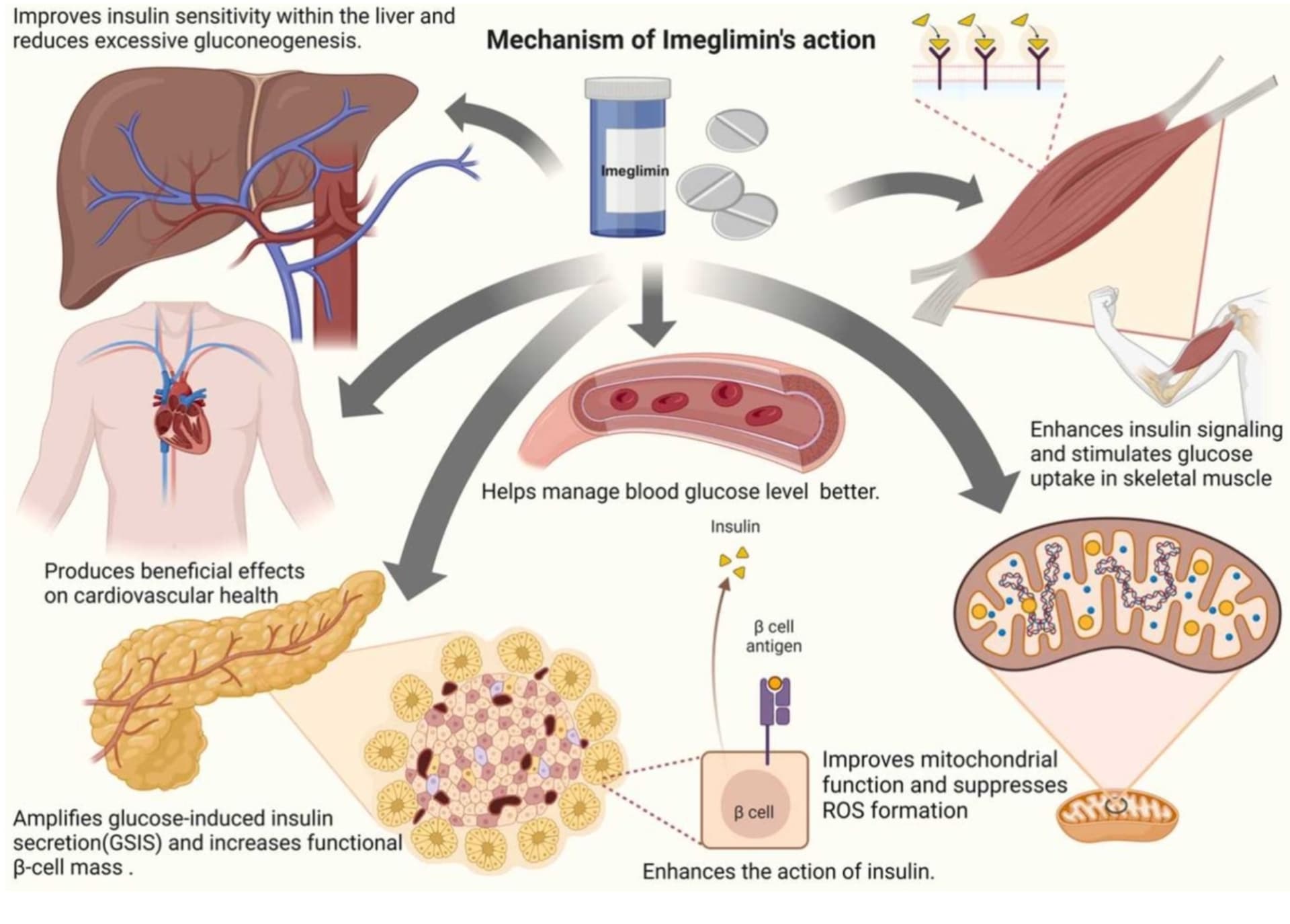
Imeglimin Amplifies Glucose-Stimulated Insulin Release from Diabetic Islets via a Distinct Mechanism of Action
https://www.biorxiv.org/content/10.1101/2020.10.20.346841v1
Does that mean you should add imeglimin to your drug stack if you have elevated A1c? Not necessarily. Let us go back to a fundamental concept, frequently invoked by Ralph DeFronzo, that diabetes (and prediabetes is just along the spectrum of poor glucose control) is a multifactorial disease with many causes, as in the defect may be along any pathway of glucose control. If it so happens, that your poor glucose control is down to a specific defect in the beta cell pathway that imeglimin addresses, you are golden: go take this drug. But that may not be the case at all. For example, many prediabetics, or even people who are normoglycemic have very high insulin levels. Clearly their problem is not an inadequate production or release of insulin by the pancreas. In that scenario, trying to fix a non-existant defect in the pancreas with imeglimin as a way to normalize glucose metabolism might not yield the desired results. Addressing any disease starts with the correct diagnosis. You must establish - and the more precisely the better - where does the defect in glucose metabolism lie in your case. And once you’ve established that, you can try to address it with the appropriate drug.
Unfortunately, we face two problems. Problem one, is that we often are not sure where the problem lies, and problem two is that a given drug may have MOA that is not transparent to us, or has multiple pathways (a “dirty” drug, like metformin). Sure, you can say metformin/sglt2i/pio/glp-1ra “brings down A1c” - but if that’s all the study shows, you really can’t be sure that it will work for you or indeed that it is appropriate and not counterproductive.
Just as an example, I take myself. My A1c is consistently high (5.7-5.9). My morning fasting blood glucose is also high (~110mg/dL). However, my insulin levels are also high. It doesn’t seem like the problem for me is inadequate insulin release. For the amount of insulin I pump out, my glucose levels ought to be lower (HOMA-IR 1.7 in my case) as reflected by A1c. I therefore am going to hold off on imeglimin for the time being. It seems to me, the problem here is somewhere else - either insulin sensitivity or excessive hepatic neoglucogenesis. That would make pioglitazone more interesting to me (in my case). But the complication is of course that imeglimin also works along multiple pathways muddying the issue - is it worth hammering the pancreas with an unnecessary “fix” because the drug also suppresses hepatic neoglucogenesis? Maybe. Or maybe I’d prefer a more targeted intervention, a drug that addresses my defect and not anything else (maybe a luxury I don’t have!).
My point here is this: we often read that a given drug does something (lowers glucose, A1c, lipids, homocysteine whatnot) and we decide to spring for it, especially if we suffer from some issue (excessive glucose levels, lipid levels whatnot). But that may transpire to be a very unwise choice.
Instead you need to ask: given my problem (say, glucose control) - will drug X (say, imeglimin) help in my case? Unless you know, why take the drug? What is the MOA of that drug and what is your defect and etiology of your pathology, does that drug address it, or does it merely give you side effects without benefits or merely surface benefits which are disastrous longer term (insulin therapy for some T2DM cases). Perhaps imeglimin might work short term - but will it work for you long term, or be counterproductive?
And that’s why I’m interested in the MOA of this drug. And why it takes me a long time to research a drug before I even consider taking it. YMMV.
 Approved Japanese Prescribing Information (Summary)
Approved Japanese Prescribing Information (Summary)